[level-membership-for-gastroenterology-and-hepatology-category]CASE 110

History: A 55-year-old man presents for annual surveillance scan.
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in the figures? (Choose all that apply.)
2. What is the most common radiologic appearance of lymphoma of the small bowel?
3. What is the most common primary site of involvement of the gastrointestinal tract with lymphoma?
4. Which of the following predisposing conditions carries the greatest risk of developing lymphoma?
D. Systemic lupus erythematosus
ANSWERS
CASE 110
Small Bowel Lymphoma
1. B, C, D, and E
2. B
3. A
4. C
References
Buckley JA, Fishman EK. CT evaluation of small bowel neoplasms: spectrum of disease. Radiographics. 1998;18:379–392.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 129.
Comment
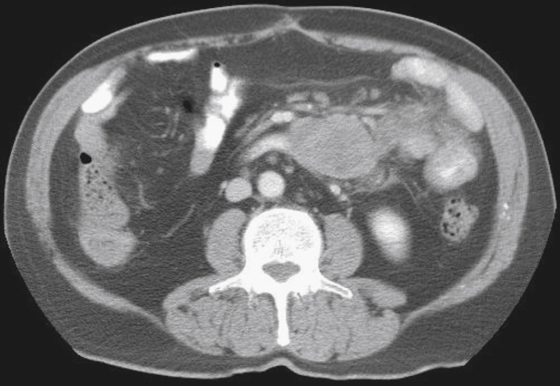
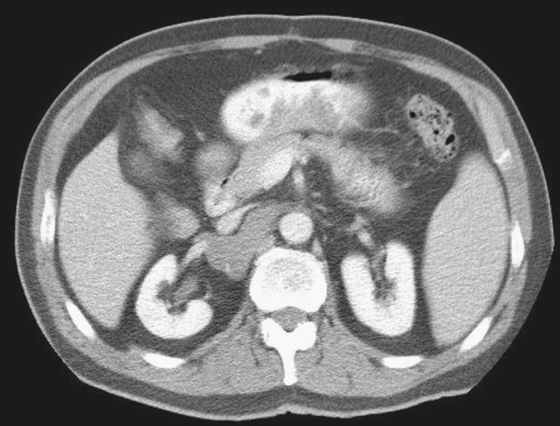
Lymphomas occur most commonly in the distal small bowel (compared with adenocarcinoma, which is proximal), but they occur infrequently in other parts of the small bowel. A feature of lymphoma is that it is often multicentric in location (see figures). The majority of small bowel lymphomas are the non-Hodgkin’s type, with Hodgkin’s disease of the small bowel being considered rare.
Lymphoma is difficult to characterize because of its variable morphologic appearance. Radiologic features include multiple nodules, solitary masses with an excavated cavity that acts as the bowel lumen, infiltrating tumors, and predominant mesenteric masses. The infiltrating or the endoexenteric mass is believed to be the most common type. The excavating form, or aneurysmal dilation, is produced when lymphoma infiltrates, replaces the muscular layer, and destroys the nerves in the area. This results in bulging of the abdominal wall, with resultant dilation. The bowel wall can become completely replaced by tumor with a persistent irregular lumen. Because of this unusual scenario, large masses of the small bowel show no evidence of bowel obstruction. However, perforation is a possibility. The bowel lumen and various layers of the bowel wall can grow back with therapy.
A variety of conditions can lead to the development of lymphoma. Any type of immunosuppression, such as that associated with AIDS, can lead to lymphoma. Perhaps at highest risk are transplant recipients, who are 50 to 100 times more likely to develop lymphoma compared with the general population. Many of these patients have an associated infection with the Epstein-Barr virus. Other conditions that increase the incidence of small bowel lymphoma include celiac disease (sprue) and systemic lupus erythematosus.
[/level-membership-for-gastroenterology-and-hepatology-category][not-level-membership-for-gastroenterology-and-hepatology-category]CASE 110
History: A 55-year-old man presents for annual surveillance scan.
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in the figures? (Choose all that apply.)
2. What is the most common radiologic appearance of lymphoma of the small bowel?
3. What is the most common primary site of involvement of the gastrointestinal tract with lymphoma?
[/not-level-membership-for-gastroenterology-and-hepatology-category]
