[level-membership-for-gastroenterology-and-hepatology-category]CASE 11

History: A 30-year-old woman with weight loss of unknown etiology presents with symptoms of bloating and abdominal distention soon after eating.
1. Which of the following should be included in the differential diagnosis for this lesion? (Choose all that apply.)
A. Superior mesenteric artery (SMA) syndrome
2. The duodenal obstruction is worse with the patient in the supine position, and relieved when the patient is placed erect or prone. What syndrome does she have?
A. Superior mesenteric artery (SMA) syndrome
3. There are types of patients who are most susceptible to this condition. Which of the following is not a predisposing condition?
A. Young women with eating disorders
E. Severe illness and sudden weight loss
4. Regarding the SMA syndrome, which of the following statements is true?
A. The normal aortomesenteric angle is at least 25 to 30 degrees.
B. Females are affected more than males.
C. The treatment of choice is surgical bypass.
ANSWERS
CASE 11
Superior Mesenteric Artery Syndrome
1. A, C, D, and E
2. A
3. D
4. B
Reference
Dahnert W. Radiology Review Manual. 5th ed. Philadelphia: Lippincott Williams & Wilkins; 2003. p 861
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 90.
Comment
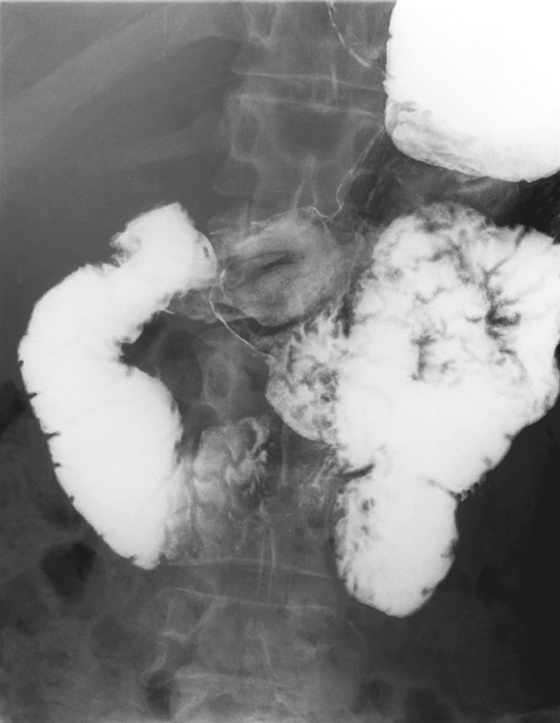
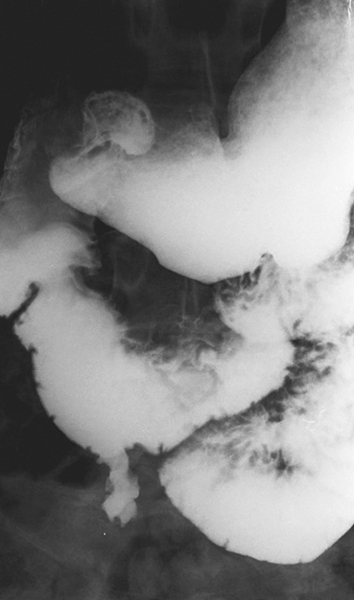
The transverse retroperitoneal portion of the duodenum is nestled in an angle created by the aorta posteriorly and the superior mesenteric artery anteriorly (see figures). This angle can vary in size, and hence this condition is sometimes controversial. Some refuse to accept that SMA syndrome is a real condition. Given the narrowness of the angle we are now able to measure on multidetector computed tomography (MDCT) sagittal images in asymptomatic patients, this is quite understandable. However, from time to time we are faced with the so-called SMA syndrome, and its symptoms and findings cannot be denied. Patients complain of abdominal pain, nausea, weight loss, and especially vomiting. Imaging of the abdomen often shows a dilated stomach and proximal duodenum. The duodenum is narrowed at the level of the aortic-SMA angle and the distal duodenum has a normal caliber.
MDCT sagittal imaging now permits us to measure the angle. An abnormal angle of less than 25 degrees is required to establish a diagnosis of SMA syndrome. In severe unremitting cases, surgical intervention, such as gastrojejunostomy, may be required.
[/level-membership-for-gastroenterology-and-hepatology-category][not-level-membership-for-gastroenterology-and-hepatology-category]CASE 11
History: A 30-year-old woman with weight loss of unknown etiology presents with symptoms of bloating and abdominal distention soon after eating.
1. Which of the following should be included in the differential diagnosis for this lesion? (Choose all that apply.)
A. Superior mesenteric artery (SMA) syndrome
2. The duodenal obstruction is worse with the patient in the supine position, and relieved when the patient is placed erect or prone. What syndrome does she have?
A. Superior mesenteric artery (SMA) syndrome
[/not-level-membership-for-gastroenterology-and-hepatology-category]
