CASE 11


History: No patient history is available.
1. What should be included in the differential diagnosis? (Choose all that apply.)
B. Doxorubicin (Adriamycin) therapy
C. Amyloidosis
D. Uremia
2. Which cardiac structure is calcified?
A. Endocardium
B. Epicardium
D. Pericardium
3. What is the most likely diagnosis if this patient presented with progressive dyspnea, ascites, and lower extremity edema?
D. Hypertrophic cardiomyopathy
ANSWERS
Reference
Wang ZJ, Reddy GP, Gotway MB, et al. CT and MR imaging of pericardial disease. Radiographics. 2003;23 Spec No:S167–S180.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, pp 269–276.
Comment
Imaging
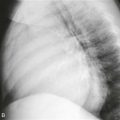
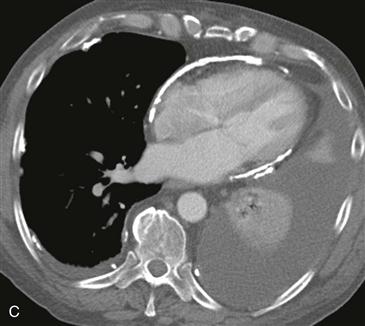
Chest radiograph shows a large left pleural effusion and extensive pericardial calcification, best visualized on the lateral radiograph (Figs. A and B). Chest CT confirms these findings and shows bilateral calcified pleural plaques indicating asbestos exposure (Fig. C). Extensive pericardial calcification is diagnostic of constrictive pericarditis in the setting of constrictive or restrictive physiology.
Differential Diagnosis
Symptoms and signs of constrictive pericarditis are nonspecific and include dyspnea, orthopnea, lower extremity edema, and ascites. CT and MRI are useful to differentiate constrictive pericarditis from restrictive cardiomyopathy. This distinction is important because treatments are vastly different. Constrictive pericarditis is treated surgically with pericardial stripping, whereas restrictive cardiomyopathy is managed medically or with heart transplantation. In patients with constrictive or restrictive physiology, ventricular filling is reduced leading to equalization of atrial and ventricular pressures. Echocardiography is unable to depict pericardial thickening accurately. Cross-sectional imaging findings of constrictive pericarditis include a pericardial thickness greater than or equal to 4 mm, pericardial calcification (Figs. B and C), and a diastolic septal bounce. Pericardial thickening may be diffuse or localized to the right heart or atrioventricular grooves.