CASE 109
History: A 43-year-old woman presents with dyspepsia.
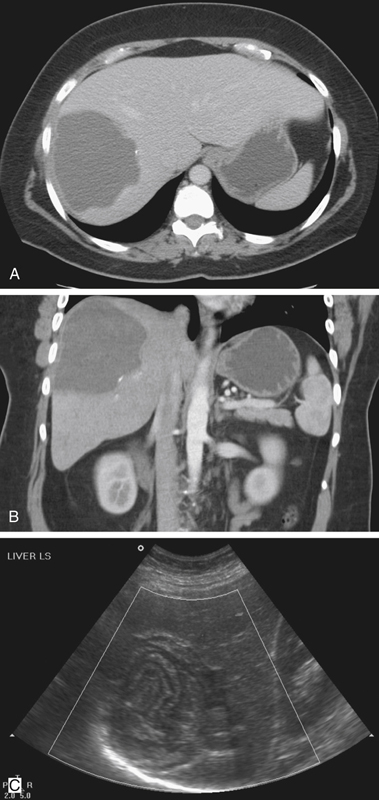
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. The hydatid cyst can rupture spontaneously. Which is the most common direction?
3. The liver is the most common site of hydatid disease involvement. What is the next most common site?
4. Which of the following statements regarding infection with Echinococcus multilocularis is true?
A. If left untreated, there is 90% mortality in 10 years.
B. Primary infection is usually asymptomatic.
C. The resultant abscess does not calcify.
D. Imaging shows multiple simple cysts.
ANSWERS
CASE 109
Hepatic Hydatid
1. B, C, D, and E
2. A
3. A
4. A
References
Beggs I. The radiology of hydatid disease. Am J Roentgenol. 1985;145:639–648.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 202.
Comment
Echinococcal cysts are produced by two types of tapeworms, Echinococcus granulosus and Echinococcus multilocularis. E. granulosus is the species most commonly seen in North America. These tapeworms live in the intestinal tract in dogs. Humans, and more commonly, sheep are the intermediate hosts, harboring the parasite in its larval stage. Humans contact the parasite by eating contaminated food, such as unwashed vegetables, or through contact with an infected dog or sheep. When the eggs of the parasite are ingested, they penetrate the mucosa of the intestine and are then carried via the portal vein to the liver. Sometimes the lungs, spleen, and kidneys are involved as well. The embryos then develop in a hydatid stage in which they form cysts in the liver. The life cycle is completed when the intermediate host dies and is consumed by the final host.
Approximately 20% to 30% of the cysts calcify, which is much higher than the percentage of simple hepatic cysts that calcify (see figures). Hydatid cysts consist of three layers. The outer pericyst is a rigid fibrous structure that is vascular and can enhance on CT. There is an intermediate layer, and finally the inner layer or endocyst is the living parasite (see figure). These cysts represent the larval stage, and there are often multiple small cysts seen within the larger cyst. Debris produced by brood capsules may be visible on the dependent potion of the cysts. Most cysts cause no symptoms until they are large enough to create pressure on adjacent structures. Sometimes the cysts spontaneously rupture into the biliary system or the peritoneal, pleural, or pericardial surfaces. Symptoms vary, but this complication can produce cholangitis or inflammation of the structures it comes in contact with. A fatal anaphylactic reaction is also possible. The plain film shown with this case is an example of chronic disease, whereas the CT image indicates a more acute stage.
Hydatid cysts must be drained for treatment. Surgery was once considered necessary treatment for this condition because of the possibility of anaphylactic reaction if the cyst drained into the peritoneum. However, it is now recognized that these cysts can be managed by percutaneous catheter drainage and instillation of scolecidal agents.






