CASE 109

1. What should be included in the differential diagnosis for the cardiac contour abnormality based on the radiograph? (Choose all that apply.)
D. Metastasis
2. Based on the CT image, what is the most likely diagnosis?
D. Metastasis
3. Which of the following features is most specific for the CT diagnosis of a false aneurysm?
B. Inferodiaphragmatic location
C. Large size
D. Disruption of the ventricular wall
4. What is the most appropriate management of a false aneurysm?
A. No therapy
C. Stent graft
D. Surgery
ANSWERS
Reference
White RD. MR and CT assessment for ischemic cardiac disease. J Magn Reson Imaging. 2004;19(6):659–675.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, pp 236–237.
Comment
Pathology and Etiology
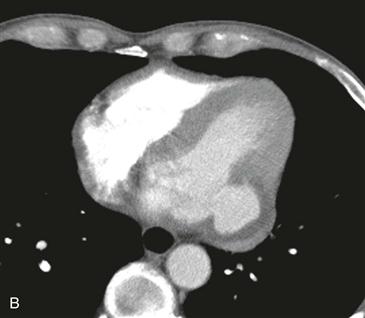
Left ventricular aneurysms result from a transmural myocardial infarction. True aneurysms have focal wall thinning and akinesis, with bulging during systole. Most true aneurysms are located in the anteroapical region of the left ventricle and have wide necks. A false aneurysm represents a contained rupture. Most false aneurysms are inferoposterior in location and are connected to the left ventricle via a narrow neck (Fig. B).
Treatment
True aneurysms are usually managed medically, unless there is substantial dysfunction, such as heart failure, arrhythmia, or peripheral embolization of thrombus. False aneurysms are usually resected because of the high risk of rupture.
Imaging and Diagnostic Criteria
With MRI or CT, true and false aneurysms can be differentiated on the basis of their necks. Location is suggestive but not definitive for differentiating a true aneurysm from a false aneurysm. The inferoposterior location of the aneurysm and the narrow neck (<50% of the diameter of the aneurysm) indicate a false aneurysm (Figs. A and B).






