CASE 108
History: A 38-year-old woman presents with chronic constipation and recent rectal bleeding.
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in the figure? (Choose all that apply.)
2. On defecography, what finding may be evident in this patient?
3. Which of the following statements regarding clinical aspects of solitary rectal ulcer syndrome is true?
A. It is mainly a disease of women.
B. A quarter of patients may be asymptomatic.
C. Patients usually present within 3 months of onset of symptoms.
D. The most common presentation is a feeling of incomplete evacuation.
4. In patients with solitary rectal ulcer syndrome, what is the most common finding on barium enema?
ANSWERS
CASE 108
Colitis Cystica Profunda
1. B, C, D, and E
2. D
3. B
4. D
References
Goei R, Baeten C, Arends JW. Solitary rectal ulcer syndrome: findings at barium enema study and defecography. Radiology. 1988;168:303–306.
Ledesma-Medina J, Reid BS, Girdany BR. Colitis cystic profunda. Am J Roentgenol. 1978;131:529–530.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, ed 3, p 300.
Comment
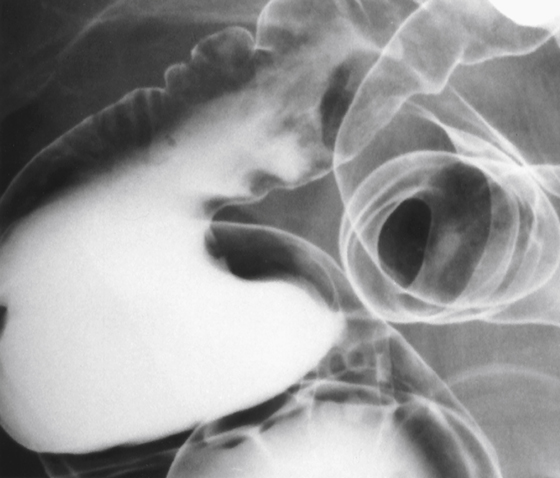
The anterior wall of the rectum is a relatively common location for pathologic findings. Probably the most common abnormalities in this area are external diseases of the cul-de-sac, including endometriosis and numerous abdominal tumors (ovarian, gastric, pancreatic, and intestinal) that produce peritoneal seeding or drop metastases to this region. All these processes have a similar appearance on barium enema. Primary tumors of the colon, mainly adenocarcinoma, can also develop in this region.
However, the anterior mucosal wall of the rectum also is a location for abnormalities that occur as the sequelae of anorectal defecation disorders. Patients with defecation problems, primarily constipation or chronic straining, can suffer from prolapse of the rectal mucosa. The anterior wall of the rectum above the peritoneal reflection is not fixed; it is free to move. This form of prolapse (or intussusception) happens every time the patient attempts to defecate. This prolapse is usually internal and difficult to document. At times even external prolapse (beyond the anal sphincter) occurs and the diagnosis becomes self-evident. Either way, the anterior wall of the rectum becomes a vulnerable structure prone to injury and induration. This, in turn, can lead to mucosal ulceration, which leads to rectal bleeding. This condition, termed solitary rectal ulcer syndrome, affects all age groups but particularly younger patients and mostly female patients.
Colitis cystica profunda is a sequela of chronic prolapse and solitary rectal ulcer syndrome. With recurrent prolapse and ulceration, there are stages of ulceration and then healing of the rectal mucosa. Over time, the regenerating mucosa can trap mucus glands underneath the mucosa. These trapped mucus glands continue to secrete mucus but do not drain because of overlying mucosa. Thus, the glands become cystic structures filled with mucin, and hence the name. With time, the cysts produce one of several polypoid structures, typically along the anterior surface of the rectum because this segment is most susceptible to this trauma. This entity is difficult to diagnose in the absence of a history of long-standing defecation dysfunction. Biopsy confirms the diagnosis, and often defecography is helpful in identifying the patient’s underlying defecation problems.