CASE 106
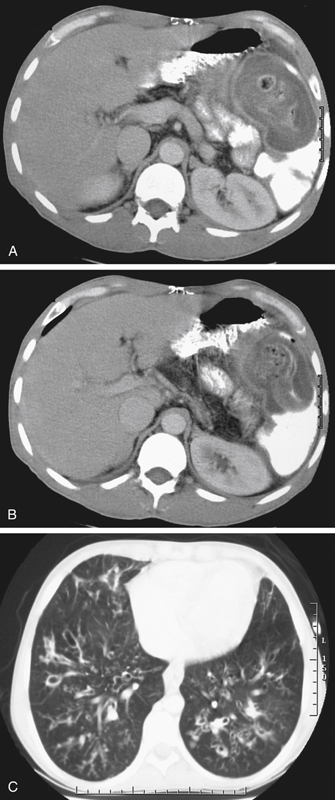
History: A 25-year-old man has been under lifelong medical care for recurrent chest infections.
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in Figure A? (Choose all that apply.)
2. Which is the most common of the following abdominal complications of cystic fibrosis?
D. Pancreatic exocrine insufficiency
3. What is the definitive treatment for cystic fibrosis?
D. There is no definitive (curative) treatment
4. Cystic fibrosis affects the pancreas in a variety of ways. Which of the following is not a pancreatic complication of cystic fibrosis?
D. Pancreatic exocrine insufficiency
ANSWERS
CASE 106
Cystic Fibrosis and Atrophy of the Pancreas
1. A, C, D, and E
2. A
3. D
4. A
References
Agrons GA, Corse WR, Markowitz RI, et al: Gastrointestinal manifestations of cystic fibrosis: radiologic-pathologic correlation. Radiographics. 1996;16:871–893.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 158.
Comment
Cystic fibrosis is a recessive genetic disorder caused by the malfunction of a single gene on chromosome 7. The gene, cystic fibrous transmembrane conductance regulator (CFTR), has to do with transport of chloride and, to a lesser extent, sodium ions from within the cell to outside the cell. There can be a variety of mutations of this gene, all resulting in the production of excessive, thick mucus within the cells of the glandular structures. This, in part, accounts for the salty skin of patients with CF. The thick mucus has its most deadly effect on the lungs, where it provides a near-perfect medium for chronic bacterial infections, which over time, distort and destroy the lung and bronchial architecture and further decrease respiratory capability.
Pancreatic involvement resulting in marked pancreatic atrophy and deficiency (such as in this case: note the absence of pancreatic tissue in its expected anatomic location) is extremely common. Supplementation with pancreatic enzymes is the common treatment along with a careful diet. With the use of CT over the years, we have come to recognize pancreatic atrophy as a common finding in older patients, with fatty infiltration of the pancreas. It seems to be a senile atrophy of the pancreas. However, the pancreatic atrophy of CF is seen in younger patients and is striking in its absence of pancreatic tissue.






