CASE 105
History: A 34-year-old woman presents with right upper quadrant discomfort.
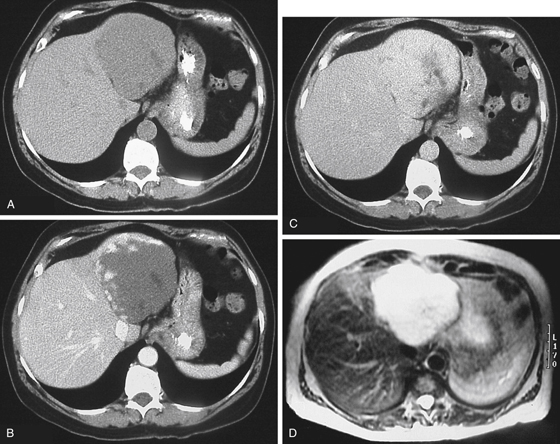
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in Figures A to C? (Choose all that apply.)
2. Which of the following statements regarding clinical features of hepatic hemangiomas is true?
B. There is equal sex incidence.
C. They are found with increasing incidence with age.
D. The most common symptom is right upper quadrant discomfort.
3. Which of the following imaging descriptions suggest hepatic hemangioma?
A. On ultrasound, they are usually hypoechoic with slight distal acoustic enhancement.
B. On CT, centrifugal progressive enhancement is diagnostic.
C. On MRI, marked hyperintensity on T1-weighted images is characteristic.
4. Hemangiomas are usually asymptomatic. What is the rare syndrome with associated thrombocytopenia?
A. Klippel-Trenaunay-Weber syndrome
ANSWERS
CASE 105
Hepatic Hemangioma
1. A, B, D, and E
2. A
3. D
4. C
References
Ros PR, Taylor HM. Benign tumors of the liver. In: Gore RM, Levine MS, eds. Textbook of Gastrointestinal Radiology. 2nd ed. Philadelphia: WB Saunders; 2000:1487–1522.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 186.
Comment
Hemangiomas of the liver, unlike those of the rest of the gastrointestinal tract, are a common finding. In the rest of the gastrointestinal tract, they are rare lesions. There is no malignant potential associated with this lesion. The problem is one of attempting to distinguish the harmless hemangioma from other lesions such hepatic metastatic disease. There are two different types of hemangiomas to consider: simple hemangioma (by far the most common) and cavernous hemangioma, such as is seen in this case. Hemangiomas of the liver are the most common benign neoplastic tumors of the liver. It is thought that these tumors affect at least 2% to 5% of the population. They are more common in women and occur most commonly in the right lobe of the liver. Multiple hemangiomas occur in 10% to 15% of these patients. By themselves, hemangiomas are rarely symptomatic and are of no consequence to the patient. Their importance lies more in the fact that their appearance can mimic that of more sinister conditions of the liver, such as metastases or malignant tumors.
Most discussions regarding hemangiomas concern the diagnostic tests that can help distinguish them from other lesions. Dynamic scanning of the liver by CT is quite helpful. In this case, initial CT scans show the hemangioma to be a low-attenuation lesion in the liver. Delayed images of the lesion over the next several minutes demonstrate increasing opacification of the hemangioma from the periphery toward the center, the centripetal opacification. However, not all cavernous hemangiomas show the classic findings, and often other studies are required. Ultrasound often shows a well-defined echogenic lesion, although the findings are not always pathognomonic. MRI is often useful because hemangiomas have a high signal intensity on T2-weighted images, but cysts and even some metastatic lesions can have a similar appearance. Radionuclide scanning is quite helpful for evaluating the liver hemangioma. On tagged red blood cell studies the hemangioma typically appears as a cold defect during the early scans, but in later images the lesion fills in and actually has increased activity on delayed images. With all these imaging studies, the greatest difficulty is encountered when the hemangioma has a central area of necrosis or fibrosis (see figures), which can mimic other lesions.






