CASE 104
History: A 53-year-old man presents with dysphagia since childhood.
1. Which of the following should be included in the differential diagnosis of the imaging finding shown in the figures? (Choose all that apply.)
2. Ingestion of which of these caustic agents produces the worst outcomes?
3. What is the potentially fatal complication of esophageal corrosive injury?
4. Which of the following obstructive lesions of the esophagus is usually not found in the proximal or mid esophagus?
C. Cricopharyngeal incoordination
D. Drug (medication) ingestion
ANSWERS
CASE 104
Esophageal Strictures from Ingestion of a Caustic Substance
1. B and C
2. A
3. C
4. A
Reference
Luedtke P, Levine MS, Rubesin SE, et al: Radiologic diagnosis of benign esophageal strictures: a pattern approach. Radiographics. 2003;23:897–909.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 17.
Comment
Ingestion of alkaline (lye) or acid substances may be either intentional or, in rare cases, accidental. Many household cleaners contain alkali or caustic substances. The degree of injury that occurs in the gastrointestinal tract is related to both the concentration and the volume of the ingested substances. The immediacy of treatment also has a significant impact regarding the sequelae of this injury. Alkaline substances produce coagulative necrosis and tend to cause a more deeply penetrating injury to the bowel.
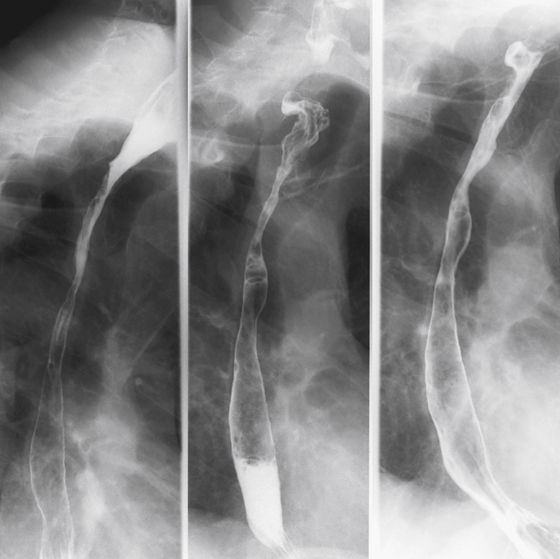
Radiologic studies may be performed (but are not recommended in known cases of caustic ingestion) as long as there are no signs of perforation, such as a widened mediastinum, soft tissue emphysema, or intraperitoneal air. Initial radiologic assessment may be performed before endoscopy is attempted and should be done with water-soluble contrast agent followed by thin barium. In the early stages (less than 12 hours after the ingestion) the only apparent problem may be a motility disorder, ranging from spasm to atony and even dilation. If there has been a severe caustic burn, superficial ulceration may be apparent in the mucosa. Over the ensuing days, the damaged mucosa sloughs and becomes edematous, with the most severe changes subsiding after several days. Radiologic examination typically is not performed during this time unless there is suspected perforation. A water-soluble study can show the location and size of the leak. The final phase of scarring, fibrosis, and stricture formation takes several weeks to months to develop. Not all patients develop esophageal stricturing, but it is more common in patients who ingested lye than in those who ingested acid. The strictures that are apparent can be either long and diffuse or weblike areas of narrowing (see figure). A significant number of these patients have developed, over time, squamous cell carcinoma of the esophagus, a well-known complication of lye ingestion.
Ingestion of alkaline and acid substances can involve the stomach, usually in the distal antrum along the greater curvature, which is where the ingested substance often comes to rest when the patient is upright. The degree of gastric injury is usually worse with ingestion of acids. The appearance looks almost identical to a malignancy: a large ulcerated mass on the greater curve of the stomach. Alkaline substances may be neutralized by the gastric acidity. However, up to 20% of patients who ingested lye develop gastric injury.






