CASE 103

1. What etiologies can cause the cardiac finding? (Choose all that apply.)
A. Trauma
C. Barotrauma
D. Surgery
2. What is the most common cause of this finding in adults?
A. Trauma
C. Barotrauma
3. Which additional finding does this patient have?
4. How can barotrauma result in pneumopericardium?
A. Interstitial air dissects along the pulmonary vessels.
B. Pneumoperitoneum occurs and communicates with the pericardium.
C. Pneumothorax occurs and communicates with the pericardium.
ANSWERS
Reference
Katabathina VS, Restrepo CS, Martinez-Jimenez S, et al. Nonvascular, nontraumatic mediastinal emergencies in adults: a comprehensive review of imaging findings. Radiographics. 2011;31(4):1141–1160.
Comment
Etiology
Pneumopericardium is most commonly posttraumatic or iatrogenic in origin. After pericardiocentesis, a small amount of air is frequently seen in the pericardium, but a large pneumopericardium is unusual. Open heart surgery is another common cause of pneumopericardium. Other thoracic surgeries are less common.
Barotrauma-induced pneumopericardium is most frequently seen in children. Although rare in adults, barotrauma can result in a large pneumopericardium. Barotrauma causes alveolar rupture. Air dissects medially along the pulmonary vessels and bronchi toward the mediastinum. It most frequently causes pneumomediastinum but may also lead to pneumopericardium. In this setting, the pneumopericardium is usually self-limiting and resolves spontaneously.
In rare instances, an esophageal-pericardial fistula can develop, sometimes secondary to a malignant tumor. In this setting, patients may have a hydropneumopericardium.
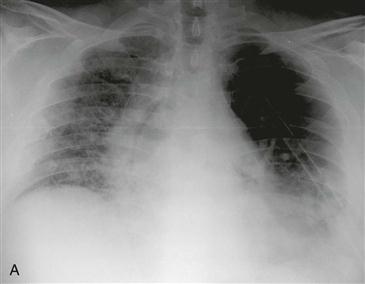
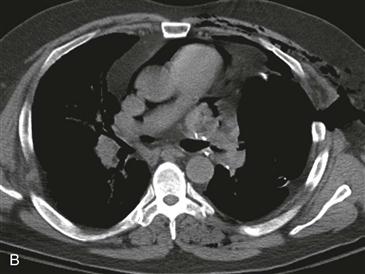
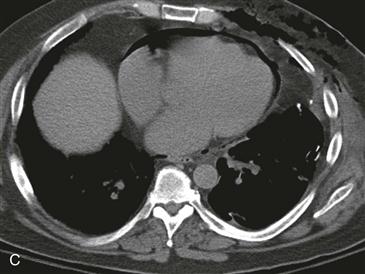
Imaging
Radiography and CT can show the air in the pericardial space (Figs. A–D). Tension pneumopericardium is a life-threatening condition that is diagnosed in the setting of hemodynamic collapse. Imaging findings on CT or MRI that suggest tamponade physiology include compression of the anterior aspect of the heart, dilated inferior vena cava, and compression or displacement of cardiac chambers. Immediate pericardial decompression is required in patients with cardiac tamponade to prevent death.






