CHAPTER 10 Volatile Anesthetics
2 What are the chemical structures of the more common anesthetic gases? Why do we no longer use the older ones?
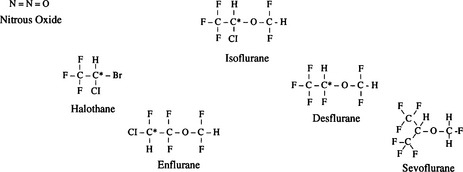
Isoflurane, desflurane, and sevoflurane are the most commonly used volatile anesthetics. As the accompanying molecular structures demonstrate, they are substituted halogenated ethers, except halothane, a halogenated substituted alkane. Many older anesthetic agents had unfortunate properties and side effects such as flammability (cyclopropane and fluroxene), slow induction (methoxyflurane), hepatotoxicity (chloroform and fluroxene), nephrotoxicity (methoxyflurane), and the theoretic risk of seizures (enflurane) (Figure 10-1).
5 Define partition coefficient. Which partition coefficients are important?
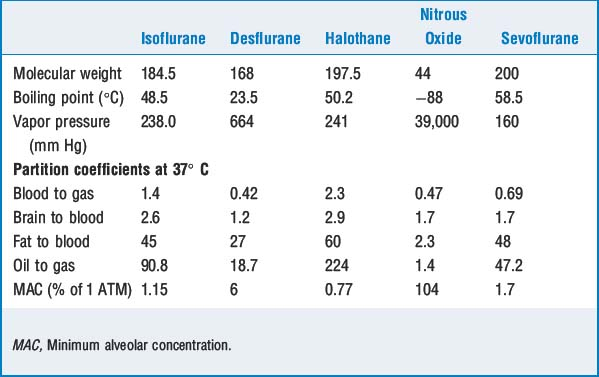
Other important partition coefficients include brain to blood, fat to blood, liver to blood, and muscle to blood. Except for fat to blood, these coefficients are close to 1 (equally distributed). Fat has partition coefficients for different volatile agents of 30 to 60 (i.e., anesthetics continue to be taken into fat for quite some time after equilibration with other tissues) (Table 10-1).
6 Review the evolution in hypothesis as to how volatile anesthetics work








7 What factors influence speed of induction?
Factors that increase alveolar anesthetic concentration speed onset of volatile induction:



Factors that decrease alveolar concentration slow onset of volatile induction:




8 What is the second gas effect? Explain diffusion hypoxia
KEY POINTS: Volatile Anesthetics 
9 Should nitrous oxide be administered to patients with pneumothorax? Are there other conditions in which nitrous oxide should be avoided?
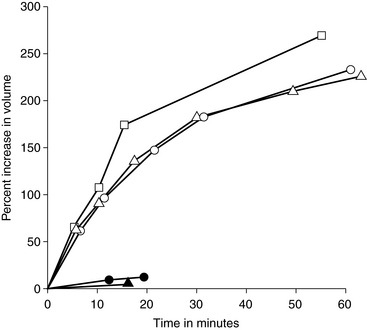
Although nitrous oxide has a low blood-to-gas partition coefficient, it is 20 times more soluble than nitrogen (which comprises 79% of atmospheric gases). Thus nitrous oxide can diffuse 20 times faster into closed spaces than it can be removed, resulting in expansion of pneumothorax, bowel gas, or air embolism or in an increase in pressure within noncompliant cavities such as the cranium or middle ear (Figure 10-2).
11 What effects do volatile anesthetics have on hypoxic pulmonary vasoconstriction, airway caliber, and mucociliary function?
16 Which anesthetic agent has been shown to be teratogenic in animals? Is nitrous oxide toxic to humans?
1. Campagna J.A., Miller K.E., Forman S.A. Mechanisms of actions of inhaled anesthetics. N Engl J Med. 2003;348:2110-2124.
2. Coppens M.J., Versichelen L.F.M., Rolly G., et al. The mechanism of carbon monoxide production by inhalational agents. Anaesthesia. 2006;61:462-468.
3. Eger E.I.II, Saidman L.J. Hazards of nitrous oxide anesthesia in bowel obstruction and pneumothorax. Anesthesiology. 1965;26:61-68.
4. Myles P.S., Leslie K., Chan M.T.V., et al. Avoidance of nitrous oxide for patients undergoing major surgery. Anesthesiology. 2007;107:221-231.
5. Sanders R.D., Weimann J., Maze M. Biologic effects of nitrous oxide. Anesthesiology. 2008;109:707-722.
