TOPIC 10 Therapeutic drug monitoring
Introduction
Indication for TDM
When to measure the drug level
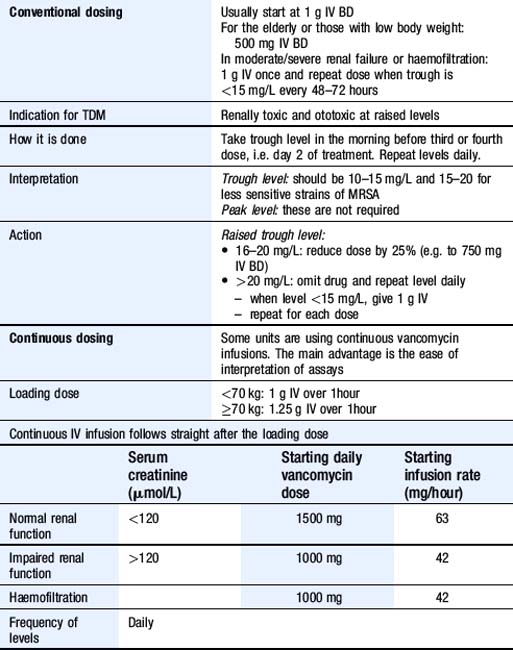
Gentamicin
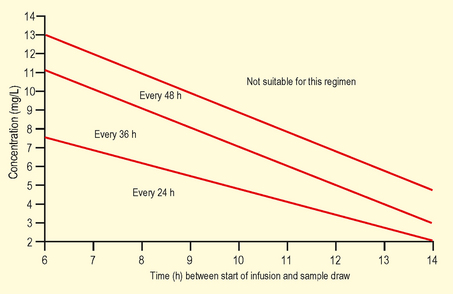
There are two methods of gentamicin dosing, the ‘conventional’ method and the ‘once-daily’ method (Table 10.1). ‘Once-daily’ is extremely dangerous if used in patients with renal dysfunction, for this reason, some units only use ‘conventional’ dosing.
| Conventional dosing | 1–1.5 mg/kg IV with frequency depending on estimated creatinine clearance (CrCl). If CrCl: |

Digoxin
See Table 10.2 for the dosing regimen, and Box 10.1 for drugs that can increase or reduce levels of the drug.
| Loading dose |
Patient toxic but levels within therapeutic range:
Patient clinically undertreated, and levels low:
Phenytoin
See Table 10.3 for the dosing regimen, and Box 10.2 for drugs that can increase or reduce levels of the drug.
| Loading dose | 15 mg/kg IV: maximum rate of 50 mg/minute |
|---|---|
| Maintenance dose |
Patient fitting and levels low:
Patient fitting and levels are in the therapeutic range:
Before you make a dose change, seek expert advice!
Theophylline/aminophylline
See Table 10.4 for the dosing regimen. Serum levels predict the type of adverse effects well, but are less good at predicting severity. Adverse effects of these drugs are outlined in Table 10.5.
| Loading dose | Aminophylline 5 mg/kg IV over 20 minutes |
|---|---|
| Maintenance dose |
Table 10.5 Levels associated with adverse effects of aminophylline and theophylline
| Level (mg/L) | Adverse reaction | Frequency (%) |
|---|---|---|
| <5 | Usually absent | N/A |
| 5–20 | Nausea and vomiting | 5–10 |
| 20–35 | As above + diarrhoea, irritability, arrhythmias | 25 |
| >35 | As above + seizures | 80 |