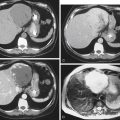
History: An 84-year-old man underwent anterior resection with primary anastomosis 8 days ago for sigmoid carcinoma. He has had ongoing confusion since the surgery. A CT scan of the abdomen is performed, including contrast through a rectal catheter.
1. Which of the following could be included in the differential diagnosis for widening of the presacral space? (Choose all that apply.)
2. Which of the following structures is the most likely to be disrupted in this patient?
3. Which of the following presacral space lesions is not an indication for percutaneous intervention?
4. What is the most common primary retrorectal tumor?
A. Adrenal rest tumor (pheochromocytoma)
D. Congenital developmental cysts
ANSWERS
CASE 10
Presacral Widening
1. B, C, D, and E
2. A
3. B
4. D
References
Bullard Dunn K. Retrorectal tumors. Surg Clin North Am. 2010;90(1):163–171.
Dahnert W. Radiology Review Manual. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2007. p 786
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, pp 315-316.
Comment
The presacral space between the midrectum and sacral bone (measured below the peritoneal reflection) can be variable and sometimes is a dilemma for radiologists. This space is taken up with fascia and some fatty tissue in most people. The measurement is valid only when the rectum is fully distended, and the lack of distention in inflammatory disease involving the rectum is usually what accounts for the widening. In Crohn’s disease, perirectal inflammatory changes are also present.
Widening can be due to processes that involve the rectum (most common), causes that affect the sacral bone, and processes that affect the retroperitoneum. Rectal causes can be both inflammatory (see figures) and neoplastic. Retroperitoneal causes can include retroperitoneal lipomatosis or fibrosis. Sacral diseases that can result in widening include sacral bony tumors (metastatic disease, as well as chordomas and neurofibromas) and sacral inflammation such as osteomyelitis.