CASE 10



1. What should be included in the differential diagnosis for Fig. A? (Choose all that apply.)
B. Enlarged main pulmonary artery
C. Thymoma
D. Sarcoidosis
2. What is the most likely diagnosis in this case?
3. Which of the following signs indicates contained or impending aortic rupture?
C. “Figure 3”
4. In which situation is earlier repair of a thoracic aortic aneurysm generally performed?
A. Asymptomatic
B. Emphysema
ANSWERS
Reference
Agarwal PP, Chughtai A, Matzinger FR, et al. Multidetector CT of thoracic aortic aneurysms. Radiographics. 2009;29(2):537–552.
Cross-Reference
Cardiac Imaging: The REQUISITES, ed 3, pp 405–408.
Comment
Imaging
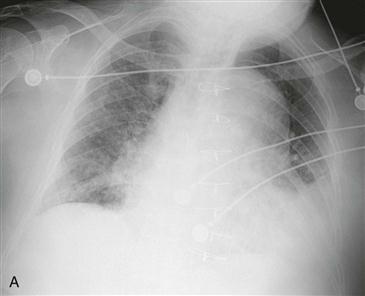
In this case, initial chest radiograph (Fig. A) shows a large left mediastinal mass with rightward tracheal displacement and a left pleural effusion. A radiograph obtained 6 hours later (Fig. B) reveals interval intubation and near-complete left hemithorax opacification. Chest CT (Fig. C) shows a distal aortic arch aneurysm. There is a large amount of left pleural fluid with high density, consistent with hemothorax and aneurysm rupture (Figs. C and D).
Prognostic Signs
The main risk associated with a thoracic aortic aneurysm is rupture. Thoracic aneurysms should be monitored yearly because of the variability in growth rate. They can rupture into the mediastinum, pleural space, pericardium, airway, or esophagus. Signs of contained or impending rupture include the “draped aorta” sign or high-attenuation blood within mural thrombus.
Management
Surgical intervention for thoracic aortic aneurysms is recommended when the risk of rupture exceeds the risk of surgical intervention. Most surgeons repair asymptomatic ascending aortic aneurysms when they attain a size of 5.5 cm and descending aneurysms when they attain a size of 6.5 cm. Earlier intervention is recommended in patients with rapid growth of the aneurysm (>1 cm/year), in patients with symptoms from the aneurysm, and in patients with Marfan syndrome.






