[level-membership-for-anesthesiology-category]
TOPIC 1 The airway
Predicting difficult airway management
Test: Bedside tests
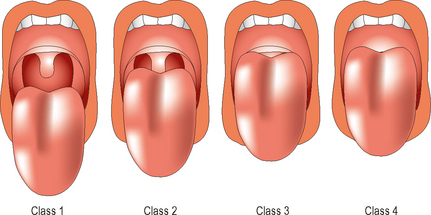
Mallampati test
How it is done
Keeping the head in a neutral position the patient is asked to open the mouth fully and protrude the tongue as far as possible, without phonation. Looking from the patient’s eye level the pharyngeal structures are inspected (Fig. 1.1). It has been suggested that the specificity and positive predictive value of the modified Mallampati test is improved by slightly extending the neck.
Limitations and complications
Protrusion of the mandible
This gives an indication of the mobility of the mandible. This can be graded as follows:
Thyromental and sternomental distance
Sternomental distance is measured from the sternum to the tip of the mandible with the head extended and is influenced by a number of factors including neck extension. It has also been noted to be a useful screening test for preoperative prediction of difficult intubation. A sternomental distance of 12.5 cm or less predicts difficult intubation.
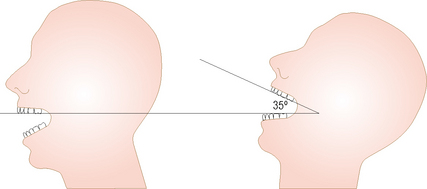
Head extension
Keeping the head in a neutral position and the line joining the mentum to the angle of the mandible parallel to the floor, the patient is asked to maximally extend the head on the neck. The angle traversed by the mento-mandibular line is measured. Head extension of 35 degrees or more is normal (Fig. 1.2).
Further investigations
View at laryngoscopy
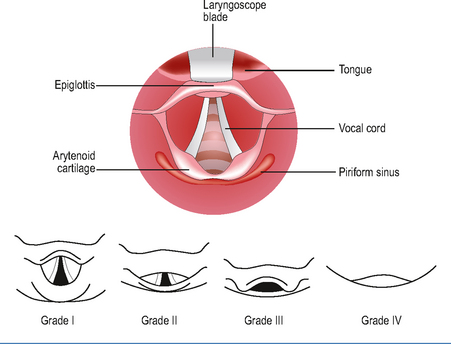
Test: Cormack and Lehane view
How it is done
Originally it was divided into four grades, depending on the view (Fig. 1.3). A modified five-grade score has also been suggested, where grade 2 is divided into 2A (posterior border of cords seen) and 2B (only arytenoids and epiglottis seen).
Other investigations of the airway
Test: Plain radiography
Patients with known conditions affecting the cervical spine, such as rheumatoid arthritis or ankylosing spondylitis should undergo lateral cervical spine radiography before intubation if at all possible. Flexion and extension views are particularly useful in this scenario (Fig. 1.4), both to detect poor neck mobility and consequent difficult direct laryngoscopy, and to pick up potentially unstable ligamentous pathology at the atlanto-axial joint.


[/level-membership-for-anesthesiology-category][not-level-membership-for-anesthesiology-category]
TOPIC 1 The airway
Predicting difficult airway management
Test: Bedside tests
Mallampati test
How it is done
Keeping the head in a neutral position the patient is asked to open the mouth fully and protrude the tongue as far as possible, without phonation. Looking from the patient’s eye level the pharyngeal structures are inspected (Fig. 1.1). It has been suggested that the specificity and positive predictive value of the modified Mallampati test is improved by slightly extending the neck.
