


History: An 80-year-old woman presents with acute abdominal pain, nausea, and vomiting. History includes a previous cholecystectomy.
1. Which is the best diagnosis based on the location of the abnormality for this patient?
2. Which choice best describes the pathological process visible on CT for this patient?
D. No etiology is demonstrated
3. The patient undergoes an enteroclysis 2 weeks later. Which choice best describes the findings?
4. At laparotomy, small bowel obstruction (SBO) was confirmed as imaged with dense adhesions the culprit. Which of the following regarding imaging of SBO is true?
A. Plain film is diagnostic in 90% of cases.
B. In ischemia, bowel wall may be hyperdense on noncontrast CT.
D. The small bowel feces sign is seen only in the setting of Crohn’s.
ANSWERS
CASE 1
Small Bowel Obstruction
1. B
2. D
3. A
4. B
References
Maglinte DD, Kelvin FM, Rowe MG, et al: Small bowel obstruction: optimizing radiologic investigation and nonsurgical management. Radiology. 2001;218:39–46.
Cross-Reference
Gastrointestinal Imaging: THE REQUISITES, 3rd ed, p 107.
Comment
Plain films of the abdomen should be the first step if bowel obstruction is suspected. The routine plain films of the abdomen are supine and upright images when possible. The classic differential air-fluid levels seen in the first 48 to 72 hours of a small bowel obstruction are almost pathognomonic of a mechanical small bowel obstruction. It is important to clearly understand what constitutes a differential air-fluid level. It represents two different air-fluid levels in the same loop of bowel. Air-fluid levels, in themselves, are nonspecific and can be seen in any number of conditions apart from mechanical obstruction. However, in mechanical obstruction, the motility of the bowel is exaggerated as it forcefully tries to push intestinal content past the narrowed segment, resulting in a to-and-fro movement of fluid. As a result there is an uneven distribution of fluid when the patient is raised to the upright position. Hence, differential air-fluid levels are seen in the same loop of bowel. With a paralytic ileus, on the other hand, the bowel movement is diminished or absent, and water distribution is equalized throughout the bowel; as a result, differential air-fluid levels are not seen.
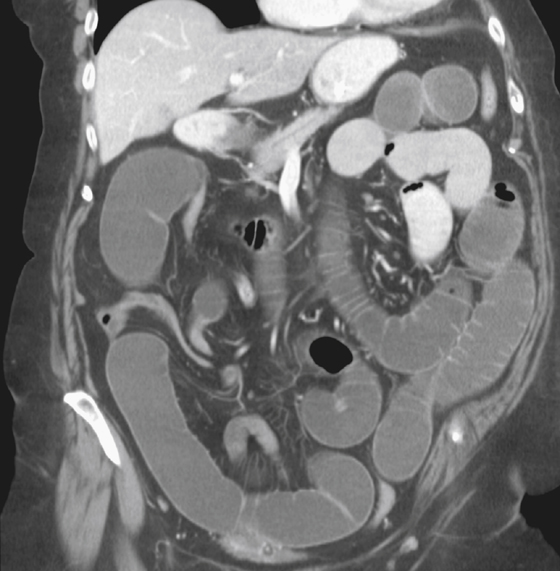
Increasingly, CT of the abdomen is being done for an abdominal complaint, especially in the acute setting. CT is able to establish the diagnosis: The findings are dilated loops of small bowel and a transition zone from dilated to collapsed loops. Occasionally the cause is demonstrated. CT is of particular value in detecting closed-loop obstruction or strangulation. CT can also identify other causes of acute abdominal pain. If the diagnosis remains unclear, barium studies (enteroclysis) may be of value to delineate the level, cause, and severity of the obstruction.






