Case 1
Raw Planar Images
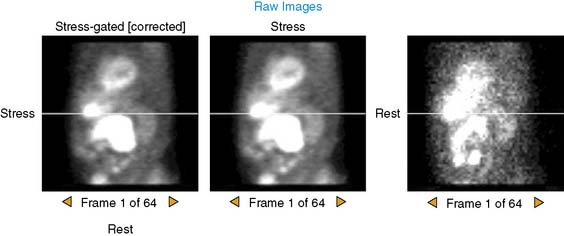
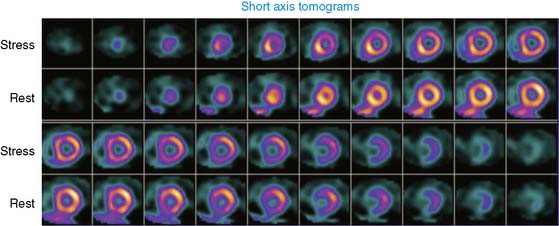
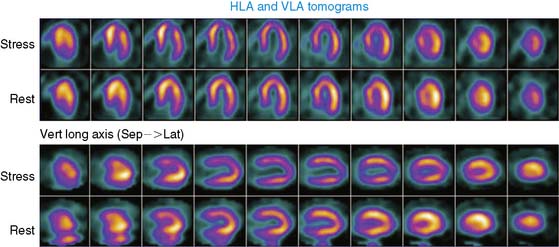
The postexercise (above) and resting (below) raw images are shown. Image quality appears adequate.
Published on 02/03/2015 by admin
Filed under Internal Medicine
Last modified 22/04/2025
Print this pageCase 1
The postexercise (above) and resting (below) raw images are shown. Image quality appears adequate.