Chapter 31 Uvulopalatopharyngoplasty – the Fairbanks technique
1 INTRODUCTION
Uvulopalatopharyngoplasty (UPPP) is generally both safe and effective as a surgical treatment for non-obese patients who suffer with mild to moderate sleep apnea and severe snoring. This refinement in surgical technique1 employs strategies for avoidance of complications and improvement of efficacy. Palatal dysfunction is avoided by minimization of soft palate shortening in the midline (uvula) area. Nasopharyngeal stenosis is avoided by minimization of posterior pillar resection and avoidance of pharyngeal undermining. Effectiveness of surgery is improved when emphasis is placed on opening the nasopharynx widely in the lateral port areas. Also, tissue removal deep in the inferior tonsillar poles (and hypopharynx) with mucosal advancement and suturing is emphasized.
1.2 OBJECTIVES
The technique described here resembles the original descriptions of Ikematsu2 and Fujita.3 However, it is modified to achieve the following desirable objectives.
2 SURGICAL PROCEDURE AND TECHNIQUE
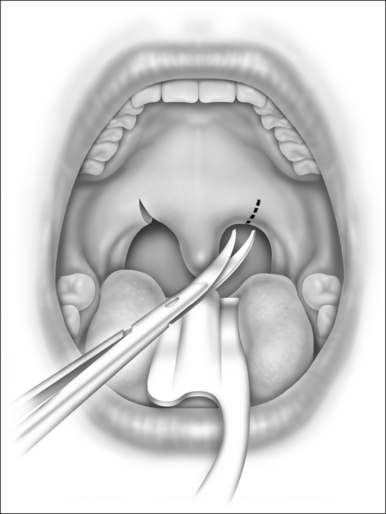
The mucosa on either side of the uvula is clamped with hemostats and then incised in an oblique direction as in Figure 31.1. This severs the drooping mucosal web between the uvula and the posterior pillar, increases the mobility of the pillar, prevents soft palatal scar contraction (with ‘tethering’), and incises some of the lowermost fibers of the nasopharyngeal sphincter. Typically, the low-hanging soft palate of an apnea patient contains few muscular fibers of the nasopharyngeal sphincter.
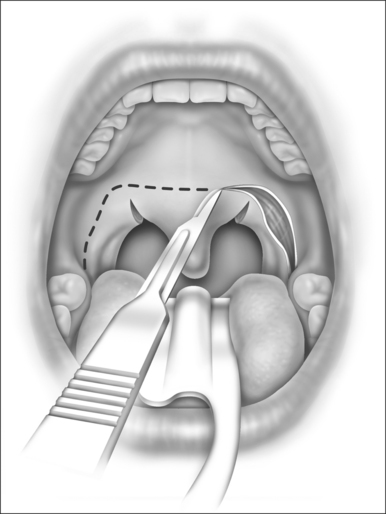
The palatopharyngeal incision is designed as three sides of a rectangle, as in Figure 31.2. It begins at the base of the tongue lateral to the inferior tonsillar pole and extends cephalad in the sulcus or angle formed between the internal surface of the mandible and the anterior tonsillar pillar. At about 1 cm above the level of the trailing edge of the soft palate, the incision makes a 90 angle, transverses the soft palate horizontally, then angles 90 downward again symmetrical to the opposite side. The ideal level for the horizontal palatal incision is at the location of the palatal ‘dimple’ as described by Dickson.4
Related posts:
 Obstructive sleep apnea: decision making and treatment algorithm
Obstructive sleep apnea: decision making and treatment algorithm
 Current techniques of adenoidectomy
Current techniques of adenoidectomy
 A minimally invasive technique for tongue base stabilization
A minimally invasive technique for tongue base stabilization
 Lateral pharyngoplasty
Lateral pharyngoplasty
 Fundamentals of minimally invasive radiofrequency applications in ear, nose and throat medicine
Fundamentals of minimally invasive radiofrequency applications in ear, nose and throat medicine
 Cautery-assisted palatal stiffening operation
Cautery-assisted palatal stiffening operation
