Thyroid nodules and goiter
A goiter is a visible swelling in the anterior neck from an enlarged thyroid gland. Derivation of the term can be traced to the French goitre, the Middle French goitron, a vulgate Latin term guttrion, and the Latin terms guttrio and guttur. Most of the terms designate the throat.
The pathogenesis for euthyroid goiter remains an enigma. Proposed mechanisms include:


 Inherited biosynthetic defects
Inherited biosynthetic defects
Regression of goiter after iodine supplementation and with thyroxine suppression of TSH supports these mechanisms. However, TSH values are not elevated in endemic goiter. Inherited biosynthetic genetic defects for thyroglobulin, thyroperoxidase, intracellular signaling pathways affecting cell life cycles, and the sodium/iodide (Na+/I−) symporter have been described.
3. Describe the natural history of diffuse nontoxic goiter.
Simple goiter tends to become multinodular over time. The nodules are heterogeneous in both morphology and function. Autonomous function, defined as TSH-independent production and secretion of thyroid hormone, can evolve. Supplementation programs in iodine-deficient populations clearly decrease the incidence of cretinism and goiter but have also increased the incidence of iodine-associated hyperthyroidism. This Jod-Basedow hyperthyroidism is more likely to occur in older people with autonomous adenomatous goiters. In the United States, this form of hyperthyroidism usually results from iodine excess due to radiographic contrast agents or medications rich in iodine. The thyroid hormone excess may be transient and may not require treatment. When it is severe, antithyroid medications and thyroidectomy can be used. Iodine excess usually precludes radioiodine as a treatment option.
4. How does lithium affect thyroid function?
Lithium has diverse effects on thyroid function. It inhibits iodine uptake, dampens iodotyrosine coupling, alters thyroglobulin structure, blocks thyroid hormone secretion, and has mitogenic effects. Both goiter and hypothyroidism can appear during prolonged exposure to lithium (Fig. 36-1).
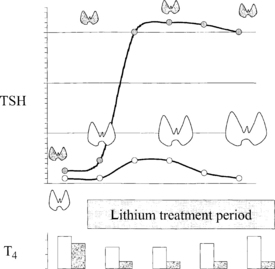
5. Describe the mechanism by which lithium produces goiter and hypothyroidism.
The inhibitory effect of lithium on thyroid hormone release provokes an increase in TSH secretion even in patients free of thyroid disease. Compensatory thyroid enlargement then occurs without the development of hypothyroidism. However, patients who have an underlying decrease in thyroid functional reserve, even if baseline thyroid hormone levels are normal, may demonstrate hypothyroidism after lithium initiation. This most commonly occurs in patients with chronic lymphocytic thyroiditis, a past history of subacute thyroiditis, or partial thyroidectomy. Because hypothyroid signs and symptoms may be difficult to decipher in the presence of depression or bipolar disorder, TSH testing before and during lithium treatment is recommended.
6. How common are thyroid nodules?
Thyroid nodules are common. Prevalence increases linearly with age. The cumulative lifetime chance of a palpable thyroid nodule approaches 6%. The prevalence at autopsy in 90-year-old subjects is about 60%. The vast majority of thyroid nodules are benign. The yield of thyroid cancer in surgical series before the widespread use of fine-needle aspiration (FNA) biopsy averaged about 10%.
7. List the differential diagnosis for a thyroid nodule.








8. Can the nature of a thyroid nodule be determined from family history?
Family history is usually not helpful. An exception is medullary thyroid cancers associated with the multiple endocrine neoplasia syndromes. Inheritance of these tumors is autosomal dominant with almost complete penetrance for the abnormal ret oncogene.
9. Do personal history and physical examination help define the nature of a thyroid nodule?
In general, no. Most patients with thyroid nodules have no symptoms and normal thyroid function. Thyroid cancer grows without causing pain. Hoarseness, dysphagia, dyspnea, and hemoptysis are rare features that suggest malignancy but also occur in benign thyroid disorders. Report of any of these symptoms by a patient with a visible goiter suggests either rapid growth or involvement of the recurrent laryngeal nerve. An aggressive form of thyroid malignancy, such as lymphoma or anaplastic thyroid cancer, is a consideration. However, both thyroid lymphoma and anaplastic thyroid cancer are rare. Other traits of nodules that suggest malignancy include size greater than 3 cm, fixation to adjacent structures, and palpable cervical lymph nodes.
10. How are most thyroid cancers discovered?
