Radical Prostatectomy

Introduction
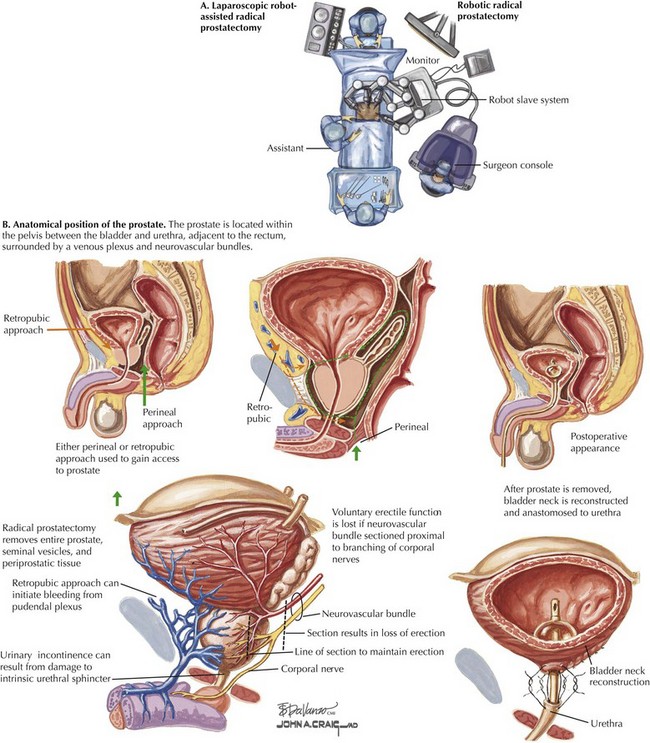
Traditionally, radical prostatectomy has been performed in the open retropubic or perineal approach. In the last decade, however, use of minimally invasive approaches has dramatically increased, particularly laparoscopic robot-assisted radical prostatectomy (Fig. 54-1, A). This approach has gained popularity because of its greater technical ease for the surgeon, especially with laparoscopic suturing, which allows for more precise suture placement during the vesicourethral anastomosis.
Prostate Cancer: Therapeutic Principles
The variation in prostate size and shape, as well as its location deep in the pelvis between the bladder and urethra and adjacent to the rectum, make surgical extirpation challenging (Fig. 54-1, B). Additionally, the prostate is surrounded by a venous plexus, and the neurovascular bundles responsible for erection run alongside the prostate. Therefore the surgical dissection required during radical prostatectomy should be performed meticulously by a surgeon with detailed knowledge of the anatomic relationships of the prostate.
Surgical Approach
Posterior Prostatic Dissection
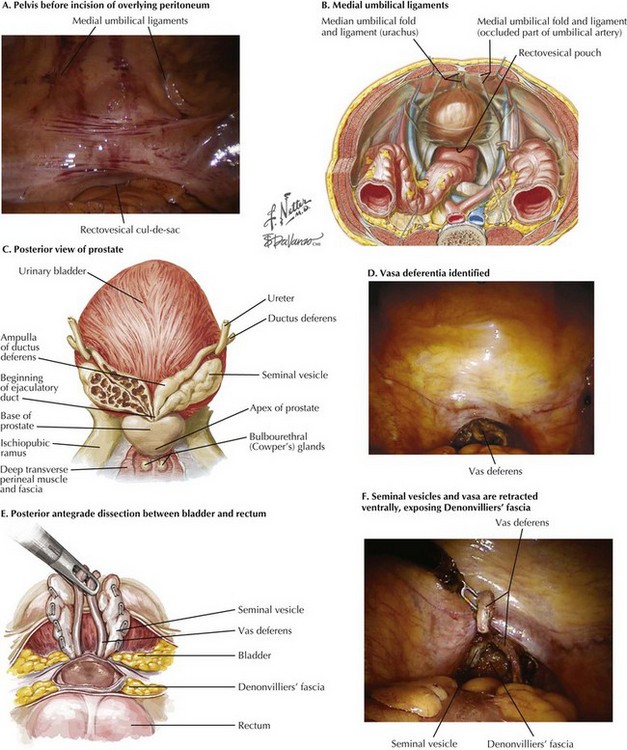
Initial inspection of the pelvis is performed to identify the relevant landmarks: the medial umbilical ligaments and the vasa deferentia. The rectovesical cul-de-sac (pouch of Douglas) is approached, and the courses of the vasa are identified through the peritoneal layer (Fig. 54-2, A-D).