Chapter 21 Penetrating Brain Injury
• In the presence of penetrating brain injury, the first step is to initiate advanced trauma life support resuscitation with early transportation to definitive care.
• The major principles of management of penetrating brain injuries include early decompression with conservative débridement of the brain. Surgeons should avoid disrupting functional eloquent cortex when chasing deep-seated fragments. In addition, it is important to identify and remove superficial expanding hematoma and foreign material, reconstruct the anterior skull base, and attempt a watertight dural closure.
• One should attempt to avoid secondary injury (i.e., meningitis, seizures, delayed vasospasm, and thromboembolic stroke) through protocol-driven neurocritical care, which includes monitoring intracranial pressure and drainage of cerebrospinal fluid.
• It is essential to maintain a high suspicion for acute and delayed neurovascular injuries (i.e., traumatic aneurysms) with subsequent endovascular evaluation and treatment when indicated.
• Delayed or immediate restoration of normal anatomy can be accomplished through craniofacial reconstruction techniques.
Historical Background
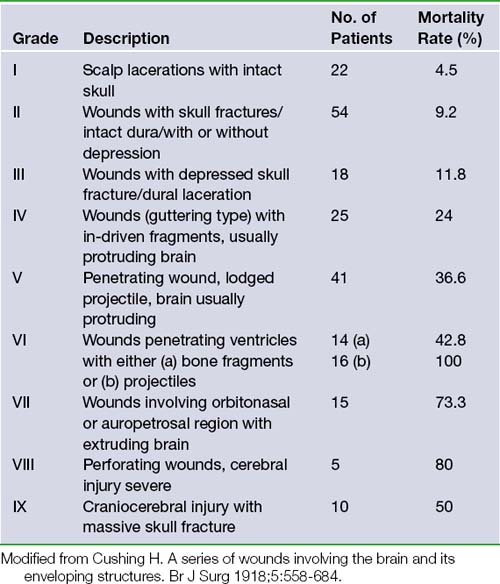
No discussion of the neurosurgical management of penetrating brain injury is complete without first acknowledging Dr. Harvey Cushing’s contributions during World War I. His landmark 1918 British Journal of Surgery article consisted of a retrospective review and classification of 219 cranial injuries and associated rates of mortality.1 In this paper he advocated aggressive débridement of necrotic tissue, removal of all in-driven debris, and meticulous scalp and dural closure. With this strategy he was able to decrease the incidence of brain abscesses and thereby lower the operative mortality rate from 55% to 29% within a 3-month period (Table 21.1).
This approach continued throughout World War II and was refined by Dr. Donald Matson in his classic monograph published in 1958.2 Matson described the principal tenets of performing initial lifesaving interventions, preventing infection, preserving neurological function, and restoring normal anatomy. These strategies hold as true today as then and have developed into modern advanced trauma life support (ATLS) guidelines,3 aseptic surgical techniques, prevention of secondary injury through neurocritical care, and craniofacial reconstruction.
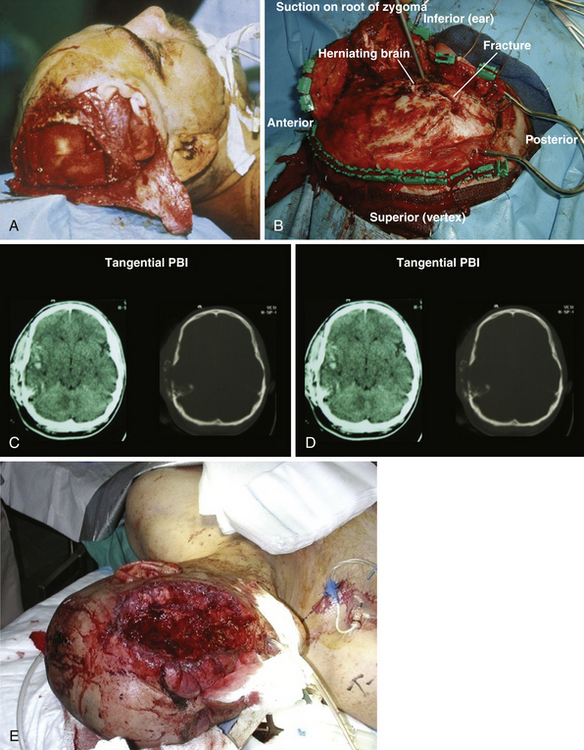
Cushing’s strategy of débridement continued to be applied in both the Korean War and the Vietnam conflict where early experiences with less aggressive approaches were met with higher infection rates and increased mortality rates.4–6 It was not until the Israel/Lebanon conflict of 1982, when computed tomography (CT) first became routine in the assessment of head injury, that a more conservative approach was advocated in favor of brain preservation. This approach was validated by 6 years of follow-up in the studies by Brandvolt and associates and Levi and colleagues and by 8 years of follow-up in a similar group of patients from the Iran-Iraq war of 1986 by Amirjamshidi and co-workers revealing no statistically significant increase in delayed infection or seizure disorders.7–9 A report of early experience with conservative débridement in Operation Desert Storm continued to find similar results10 (Fig. 21.1).
In 1995, the Brain Trauma Foundation developed the first traumatic brain injury (TBI) guidelines with the assistance of international experts in the field to address the need for protocol-driven health care based upon the most current scientific literature. In 2001, guidelines for the care of PBI were created toward the same end with the support of the Brain Injury Association, the International Brain Injury Association, the American Association of Neurological Surgeons (AANS), and members of the Congress of Neurological Surgeons (CNS). These guidelines stand as the most comprehensive evidence-based evaluation of interventions specific to the care of PBI and are summarized in Table 21.2.11 It is worth mentioning, however, that despite the exhaustive literature search used to develop the guidelines, no recommendation achieves a level beyond that of option and this underscores the need for further research. No level I or II data exist on the subject.
TABLE 21.2 2001 Guidelines for the Management of Penetrating Brain Injury
| Topic | Conclusion | Recommendation Level |
|---|---|---|
| I. Antibiotic prophylaxis | The use of prophylactic broad-spectrum antibiotics is recommended for patients with PBI. | Option |
| II. Seizure prophylaxis | The use of prophylactic antiseizure medications in the first week after PBI is recommended to prevent early post-traumatic seizures. | Option |
| III. ICP monitoring | Early ICP monitoring is recommended when the clinician is unable to assess the neurological examination accurately or if CT scans suggest elevated intracranial pressure. The need to evacuate a mass lesion is unclear. | Option |
| IV. Management of CSF leaks | Surgical correction is recommended for CSF leaks that do not close spontaneously, or are refractory to temporary CSF diversion. During the primary surgery, every effort should be made to close the dura and prevent CSF leaks. | Option |
| V. Neuroimaging | CT scanning of the head is strongly recommended. Angiography is recommended in PBI when a vascular injury is suspected. Routine MRI is not recommended for use in the acute management of missile-induced PBI. | Option |
| VII. Surgical management | Evacuation of hematomas with mass effect, conservative débridement of missile tract without retrieval of remote fragments, débridement of nonviable scalp, bone, or dura before primary closure, and watertight repair of open-air sinus injuries is recommended. | Option |
| VIII. Vascular complications | CT angiography and/or conventional angiography should be considered when vascular injury is suspected. If traumatic intracranial aneurysm (TICA) or arteriovenous fistula (AVF) is identified, surgical or endovascular management is recommended. | Option |
CSF, cerebrospinal fluid; CT, computed tomography; ICP, intracranial pressure; MRI, magnetic resonance imaging; PBI, penetrating brain injury.
Modified from Aarabi B, Alden TD, Chestnut RM, et al. Management and prognosis of penetrating brain injury. J Trauma 2001;51:3-43.
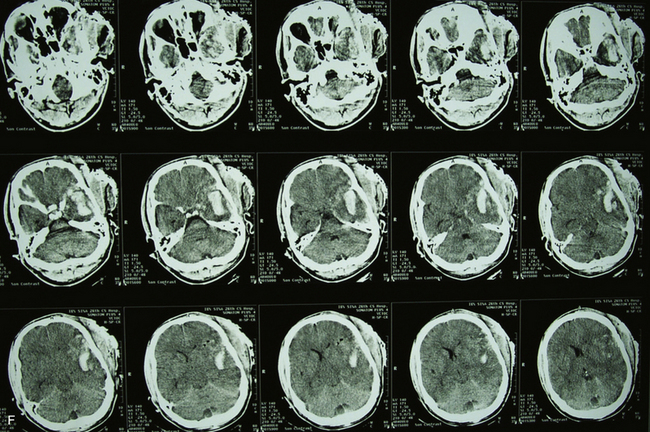
Craniofacial injuries sustained during OEF and OIF have resulted in further modifications to the management of patients with severe PBI.12–18 Although aggressive débridement of the brain is no longer used, early and aggressive cranial decompression with subsequent watertight dural closure is the current accepted practice (see Fig. 21.1).18 This strategy affords the patient protection from significant elevations in intracranial pressure (ICP) during the long flights, unaccompanied by neurosurgeons, from operative theaters back to the United States. This initial stabilization is then followed by protocol-driven neurocritical care aimed at preventing secondary neurological decline and maximizing neurological recovery. Though the data are still under review, preliminary analysis appears favorable15,19 (Fig. 21.2).
Prognosis
Civilian PBI has high mortality rates that remain refractory to medical and neurosurgical advances based on the most recent case series.20,21 The mortality rate in most retrospective cohorts is greater than 70% owing in large part to the higher percentage of gunshot wounds (see Fig. 21.2), suicides, and the ubiquitous absence of cranial protection (helmets) compared to military injuries.22–26 Other variables that differentiate these two groups are presented in Table 21.3. The reported civilian mortality rates from gunshot wounds to the head (GSWH) in the literature range from 23% to 92% with those series on the lower end including a number of cases without dural violation.27–29 Death from PBI occurs shortly after injury with 70% of patients succumbing after the first 24 hours23,25 (Table 21.4).
TABLE 21.3 Comparison of Civilian and Military Penetrating Brain Injury
| Factor | Civilian | Military |
|---|---|---|
| Population | Heterogeneous | Homogeneous (younger overall age) |
| Mechanism | Gunshot/suicide | Blast/shrapnel |
| Environment | Modern sanitation | Possibly contaminated |
| Prehospital care | Variable | Immediate |
| Tertiary care | Hours | Variable |
| Injury severity score (ISS)∗ | Low | High |
TABLE 21.4 Prognostic Variables
| Topic | Conclusion | Data Class |
|---|---|---|
| I. Age | Age > 50 years is associated with higher rate of mortality, but significance is unclear. | III |
| II. Cause of injury (suicide) | Self-inflicted GSWH carry a higher rate of mortality than those for other causes. | II |
| III. Mode of injury | Perforating wounds have a higher mortality rate than tangential or penetrating PBIs. | III |
| IV. Caliber of weapon | No demonstrated effect. | |
| V. Hypotension | Hypotension is associated with increased mortality rate. | III |
| VII. Coagulopathy | Coagulopathy is associated with increased mortality rate. | III |
| VIII. Respiratory distress | Respiratory distress is associated with increased mortality rate. | III |
| IX. GCS | In civilian injuries, low GCS score correlates with higher mortality rate and unfavorable outcome. In military injuries, low GCS score correlates with unfavorable outcome. | I (civilian) III (military) |
| X. Pupil size and response | The presence of bilateral fixed and dilated pupils is highly predictive of fatal outcome. | III |
| XI. ICP | High ICP is predictive of higher mortality rate. | II |
GCS, Glasgow Coma Scale; GSWH, gunshot wounds to the head; ICP, intracranial pressure; PBI, penetrating brain injury.
Modified from Aarabi B, Alden TD, Chestnut RM, et al. Management and prognosis of penetrating brain injury. J Trauma 2001;51:44-86.
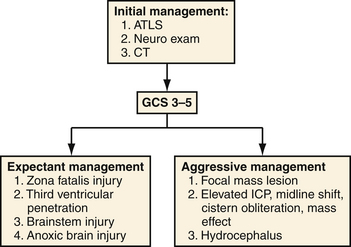
Prognostic indicators were classified as a separate section in the 2001 PBI guidelines and are summarized in Table 21.4.11 Of these factors and consistent with data in other forms of TBI, a postresuscitation Glasgow Coma Scale (GCS) score stands as the most reliable predictor of death and other unfavorable outcomes.30 This measure is a consistent predictor for both civilian and military populations but appears to have the greatest correlation with civilian mortality. In series segregating out patients with poor presenting neurological function or upon subgroup analysis of those with GCS scores of 3 to 5, mortality rate rises to 87% to 100%.25–31 A recommended triage for both military and civilian patients is located in Figure 21.3.
Because of the many dissimilar characteristics between civilian and military populations it has been difficult to correlate the weight of certain prognostic factors and to compare treatment measures across groups; however, a recent study by Dubose and associates compared the epidemiology and outcomes of military and civilian severe TBI.19 The Joint Trauma Theater Registry (JTTR) database and the American College of Surgeons’ National Trauma Data Bank (NTDB), both the largest patient databases of their kind, were queried for severe TBI and PBI. Subgroup analysis then selected for isolated PBI from gunshot wounds and statistically matched counterparts across the same period of 2003 to 2006. The results showed a threefold increase toward neurosurgical intervention in the JTTR group compared with civilian, particularly in the way of ICP monitoring (13.8% vs. 1.7%). Outcomes showed a tenfold decrease in mortality rate in the JTTR over their NTDB counterparts (5.6% vs. 47.9%). Although a dramatic difference in mortality rates between these populations is not new, this study excludes the confounding differences in explosive fragment PBI and GSWH injuries and allows for a more direct comparison of pertinent factors.
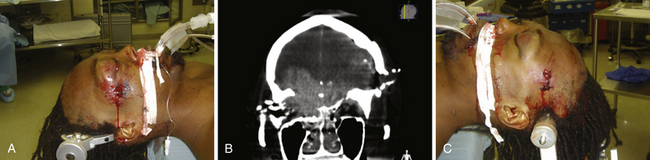
To make these populations truly comparable, however, the high rate of suicides and point-blank injuries in the civilian population needs to be accounted for in the analysis. In the most recent case series of civilian GSWH, Hofbauer and colleagues analyzed the impact of shooting distance on mortality rate in contact, near-contact, intermediate range, and at distance.21 Those at intermediate and long distances had a 0% mortality rate of 19 patients treated. In contrast, the contact group showed mortality rates of 91% with self-inflicted wounds (n = 46) and 100% with non-self-inflicted wounds (n = 4). Until variables of mechanism and modes of injury can be more appropriately matched, treatment effects across civilian and military PBI will be difficult to discern (Figs. 21.4 and 21.5).
Related posts:
 Posterior Fossa and Brainstem Tumors in Children
Posterior Fossa and Brainstem Tumors in Children
 Vascular Malformations (Arteriovenous Malformations and Dural Arteriovenous Fistulas)
Vascular Malformations (Arteriovenous Malformations and Dural Arteriovenous Fistulas)
 Basic Principles of Deep Brain Stimulation for Movement Disorders, Neuropsychiatric Disorders, and New Frontiers
Basic Principles of Deep Brain Stimulation for Movement Disorders, Neuropsychiatric Disorders, and New Frontiers
 Endoscopic Approaches to Skull Base Lesions, Ventricular Tumors, and Cysts
Endoscopic Approaches to Skull Base Lesions, Ventricular Tumors, and Cysts
 Spasticity: Classification, Diagnosis, and Management
Spasticity: Classification, Diagnosis, and Management
