CHAPTER 43 Patent Ductus Arteriosus
Patent ductus arteriosus (PDA) is defined as incomplete closure and patency of the ductus arteriosus beyond functional closure after birth. The ductus arteriosus is a vessel that extends from the anterolateral aspect of the descending thoracic aorta to the superior aspect of the main pulmonary artery, close to the origin of the left pulmonary artery. Embryologically, it is a remnant of the distal left sixth aortic arch. A normal and vital structure in the fetus, it is necessary for diverting blood flow from the main pulmonary artery to the aorta, thereby bypassing the high-resistance pulmonary circulation.1 This diversion is crucial to normal development of the right ventricle and results in passage of only 10% of the right ventricular cardiac output through the lungs. Premature closure of the ductus arteriosus in the fetus, as seen with maternal use of nonsteroidal anti-inflammatory drugs (NSAIDs), leads to right ventricular failure and fetal hydrops (Fig. 43-1).2
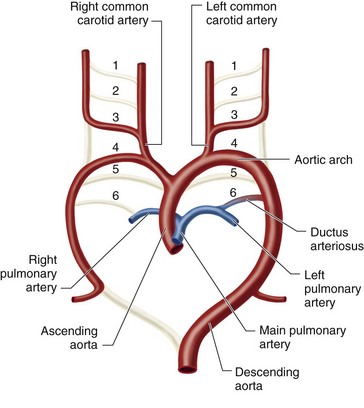
 FIGURE 43-1
FIGURE 43-1The duct functionally closes in the first 18 hours of life in full-term healthy infants. However, it fully closes several weeks later, after which it is unable to regain its patency. In premature infants, patency can be seen up to 10 days after birth.3,4 Some consider the patency abnormal only after 3 months of age. The patency causes a left to right shunt that increases pulmonary blood flow at the expense of systemic flow.5 If untreated, based on the size of the PDA, pulmonary hypertension and Eisenmenger syndrome develop in children and adults (Fig. 43-2).1
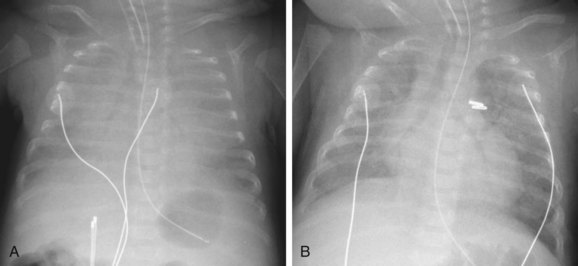
 FIGURE 43-2
FIGURE 43-2MECHANISM OF PHYSIOLOGIC CLOSURE
Histologically, the wall of the ductus arteriosus is composed of the same three layers as those of the aorta or main pulmonary artery—the intima, media, and adventitia. The media of the ductus arteriosus is different in that the smooth muscle fibers have a spiral and longitudinal orientation, instead of a concentric one, as seen in the aorta and pulmonary artery.1
Relative low oxygen tension and high levels of prostaglandin E2 (PGE2) and prostacyclin (PGI2), produced by the placenta, are responsible for the continued patency of the ductus arteriosus in the fetus. PGE2 and PGI2 interact with specific receptors in the smooth muscle layer of the media, leading to vasodilation.6
The process of closure begins at birth. The sudden increase of oxygen tension leads to influx of calcium and thereby muscle contraction in the smooth muscles of the media. Because of the metabolic breakdown of prostaglandins by the newly functioning lung and the absence of the placenta, the PGE2 and PGI2 levels fall, diminishing their vasodilation effect. Smooth muscle contraction in the ductus arteriosus wall shortens the ductus and causes luminal occlusion. In the following weeks, fibrosis ensues, leading to permanent sealing.1,6 Perinatal hypoxia impedes the natural closure process. Pharmacologic treatment of PDA is based on muscular constriction in the middle of the ductus, leading to segmental ischemia and fibrosis.3,6
PREVALENCE AND EPIDEMIOLOGY
PDA can be isolate or part of a complex cardiac malformation.7 The overall incidence in children born at term is 0.02% to 0.08%, which accounts for approximately 10% of all congenital heart disease. Most cases are sporadic. It is more common in premature and term infants with maternal rubella infection in the first trimester of pregnancy. Maternal use of amphetamine and phenytoin and fetal alcohol syndrome are also associated with PDA.8 PDA is more frequent in certain genetic syndromes such as trisomy 21, trisomy 18, 4p− syndrome, Holt-Oram syndrome, Carpenter syndrome, and Char syndrome.1,9
PDA is twice as common in females when it is isolated and sporadic; however, if associated with prematurity or prenatal infection, the frequency is equal between the genders.9 A study by Mangones and colleagues,10 which compared the prevalence of various congenital cardiovascular malformations by race and ethnicity, showed no racial preference for isolated PDA and an overall less frequency of congenital cardiac malformations in Hispanics. However, a previous study by Chavez and associates11 described an increased prevalence of isolate PDA in African Americans.
ETIOLOGY AND PATHOPHYSIOLOGY
The magnitude of left to right shunting depends on the flow resistance of the ductus arteriosus and the pressure gradient between the aorta and pulmonary artery. The flow resistance depends mainly on the diameter and length of the narrowest portion of the ductus arteriosus. The pressure gradient between the two ends of the PDA depends on the pulmonary and systemic vascular resistance and the cardiac output. The larger the diameter of the narrowest portion of the ductus, the greater the impact of changes in the systemic and pulmonary resistance on the pressure gradient and, therefore, on the magnitude of shunting. If the narrow portion is small in caliber, thereby a restrictive shunt, then the length of the narrow portion is important. A longer length of the ductus is associated with a smaller magnitude of shunting.1,6,8
The left to right shunt causes overcirculation and fluid overload of the pulmonary bed, which lead to decreased lung compliance and increased work of breathing. The shunting also causes left heart volume overload and, if the ductus is moderate to large in size, the increased left atrial and left ventricular end-diastolic pressures can eventually lead to hypertrophy of the left ventricle. The wall tension of the hypertrophied left ventricle causes catecholamine release, which results in tachycardia and therefore a shorter diastolic time. On the other hand, the diastolic blood pressure of the aorta decreases because of blood passage through the ductus during diastole. This decreased diastolic pressure and shorter diastolic time causes decreased coronary perfusion and, when combined with increased myocardial tension and oxygen demand, may result in subendocardial ischemia, which can be detected by elevated troponin levels.12
When the pulmonary arteries are subjected to long-standing increased flow and high pressure, microvascular injury develops, which leads to intimal proliferation and arteriolar medial hypertrophy. This eventually causes fibrosis and obliteration of the pulmonary arterioles and capillaries, and pulmonary arterial hypertension ensues. As the pulmonary vascular resistance gradually increases and approaches or exceeds the systemic vascular resistance, ductal shunting reverses and becomes right to left. This is called Eisenmenger syndrome.1,6,8
Clinical Features
Age of clinical presentation and presence of and type of symptoms at the time of presentation depend on the size of the PDA and pulmonary vascular resistance. The clinical presentation can vary from no symptoms, where the shunt is diagnosed incidentally, to congestive heart failure and Eisenmenger syndrome. Many patients have exercise intolerance or the diagnosis of reactive airway disease.1,8,13 Most patients compensate well, even with a moderate left to right shunt and remain asymptomatic during childhood. A well-tolerated PDA can become clinically significant when combined with effects of acquired conditions such as ischemic heart disease or calcific aortic stenosis. The hallmark physical finding is a machinery murmur, which is a continuous murmur detected at the left upper sternal border. If the shunt is moderate or large, the left ventricular impulse will be prominent and laterally displaced and the pulse pressure will be increased, resulting in a bounding peripheral pulse.
Eisenmenger syndrome presents with cyanosis and clubbing that may spare the fingers because the right to left shunting is distal to the subclavian arteries. This cyanosis may be more profound when systemic vascular resistance is decreased, such as after exercise or hot weather. On auscultation, there may be no murmur, a high-frequency diastolic decrescendo murmur of pulmonary regurgitation, and/or a holosystolic murmur from tricuspid valve regurgitation. Peripheral edema is a late manifestation caused by right ventricular dysfunction.14,15
MANIFESTATIONS OF DISEASE
Clinical Presentation
Grading
In adults, PDA is usually isolated and discovered incidentally on physical examination or during echocardiography screening. Grading of PDA is based on a combination of echocardiographic findings, physical findings on auscultation and examination, and presenting symptoms. In adults, PDA is categorized as four grades—silent, small, moderate, and large. A silent PDA is usually incidentally diagnosed on echocardiography. The patient is asymptomatic and has no audible heart murmur. A small PDA is associated with an audible continuous murmur in the left upper sternal border that radiates to the back. The patient has normal peripheral pulses and no pulmonary hypertension. In moderate PDA, there is an audible continuous murmur, wide, bouncy peripheral pulses caused by aortic regurgitation, and runoff of blood during diastole by the shunt. The left atrium and left ventricle are enlarged; the PDA is associated with pulmonary hypertension that is commonly reversible. A PDA is graded as large when signs of pulmonary hypertension have developed. The typical continuous murmur is absent. Differential cyanosis, in which the oxygen saturation of the feet is lower than that of the right arm, is typically seen. Grade 4 patients are mostly adults with Eisenmenger syndrome.14,15
Complications
The complications of PDA usually present in adulthood, when congestive heart failure presents in the third decade of life. This is caused by chronic left heart volume overload. Heart failure is associated with atrial flutter or fibrillation and is caused by left atrial dilation. This may be the first sign in these patients. Pulmonary hypertension or Eisenmenger syndrome is a manifestation of irreversible pulmonary vascular disease, seen with moderate and large PDA.1,14,16
Infective endarteritis is a significant health issue in countries where there are lower standards of health, inadequate oral hygiene, and less widespread antibiotic use. When endoarteritis develops, it occurs at the pulmonary end of the shunt, which can cause bland and septic emboli to the lungs. No systemic embolization occurs.15,16
The left recurrent laryngeal nerve passes in the triangular space created by the main pulmonary artery, aortic arch, and PDA. When pulmonary hypertension develops, the pulmonary artery becomes enlarged and this space narrows, which may cause impingement of the recurrent laryngeal nerve and development of unilateral vocal cord paralysis and hoarseness. This is a rare complication.1
Imaging Technique and Findings
Ultrasound
The diagnostic modality of choice for PDA is generally echocardiography, in which color Doppler is used to detect a PDA and used to estimate the degree of shunting. Gray-scale and M-mode echocardiography are useful for visualizing the geometry of the ductus, calculating left atrium and ventricle sizes, and quantifying the left ventricle systolic function. If Eisenmenger syndrome is present, there is a low-velocity right to left shunting, which is difficult to detect, even by color Doppler. In this case, secondary signs of septal flattening, right ventricular hypertrophy, and high-velocity pulmonary regurgitation are the findings that warrant a search for a PDA (Fig. 43-3).1,15
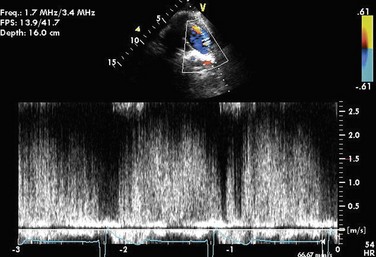
 FIGURE 43-3
FIGURE 43-3Radiography
On standard chest radiography, PDA only becomes evident when there is a moderate PDA. The left atrium and left ventricle are enlarged. In infants and children with a moderate or large PDA, shunt vascularity is seen. In patients who have Eisenmenger syndrome, the central pulmonary arteries are enlarged and there is peripheral pruning of the pulmonary arteries. In older patients, a calcification in the aortopulmonary window indicates a calcified ductus arteriosus or PDA. In such patients, the aorta may be enlarged because of the chronic right to left shunt (Fig. 43-4).17
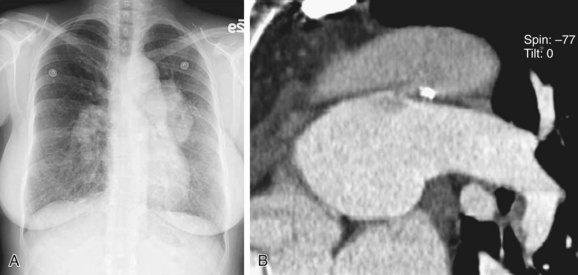
 FIGURE 43-4
FIGURE 43-4Computed Tomography
Computed tomography angiography (CTA) is useful for demonstrating the PDA, especially when it is not detectable on echocardiography, but is suspected. CTA also helps in characterizing the morphology of PDA and determining whether it is calcified, both important factors in treatment planning. Other associated vascular anomalies, such as a vascular ring or the presence of other associated congenital heart disease, can be detected by CTA. Multidetector CT (MDCT) involves faster imaging with a smaller contrast bolus, allowing increased use of this modality in the assessment of mediastinal vascular anomalies and acquired disease. The quick scanning results in fewer motion artifacts and the ability to evaluate children and older patients. The higher spatial resolution and presence of multiple rows of detectors along the longitudinal axis of the patient allow better multiplanar-reformatted and surface-shaded three-dimensional images to be created. These are most useful for quickly displaying the anatomy of the vascular abnormality and its relationship with adjacent structures. The ease of use of MDCT and its excellent depiction of anatomy has rendered CTA a common first means of evaluating for vascular anomalies in the thorax. The disadvantage of CTA is the use of intravenous iodinated contrast, contraindicated for patients with renal failure and for those who are allergic to intravenous contrast (Fig. 43-5).17–19
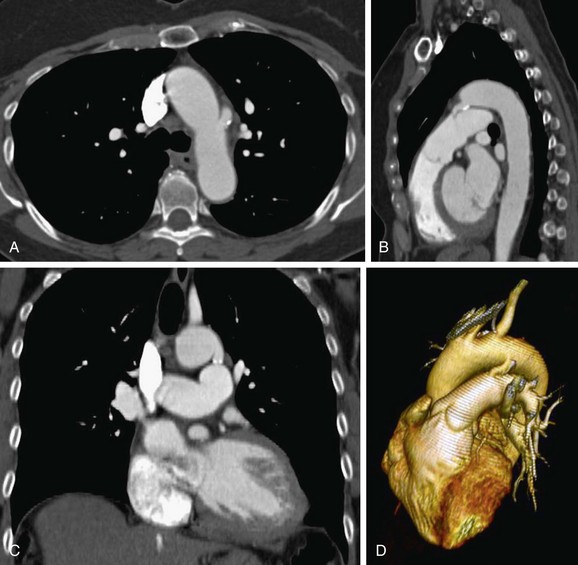
 FIGURE 43-5
FIGURE 43-5