74 Other Neuromuscular Transmission Disorders
Lambert–Eaton Myasthenic Syndrome
Etiology and Pathophysiology
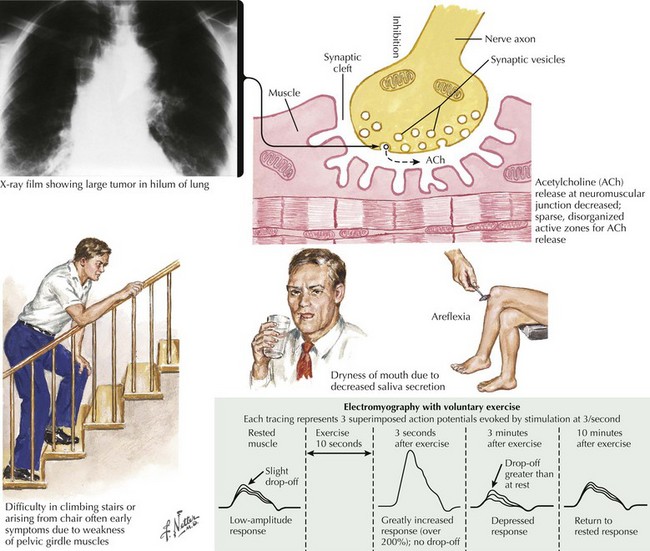
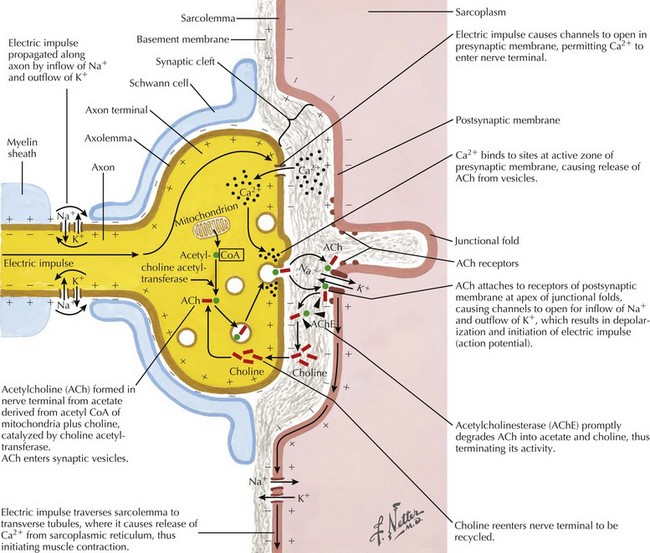
Under normal conditions, neuronal depolarization opens VGCCs on the presynaptic axon terminal membrane, resulting in calcium influx within the nerve terminal. Intracellular calcium binds to calmodulin and mobilizes acetylcholine (ACh) vesicles that are released into the synaptic cleft (Fig. 74-1). The VGCCs are the primary site of immunopathology in LEMS. Divalent IgG autoantibodies cross-link the calcium channels, disrupting their function, resulting in inadequate release of presynaptic ACh vesicles from motor and autonomic cholinergic nerve terminals. The release of fewer ACh quanta at the neuromuscular junction decreases the probability of reaching the “all or none” depolarization threshold of a muscle fiber and thus the likelihood of the muscle fiber action potential (MFAP) generation. It is this drop out of a significant number of MFAP generation that results in low CMAPs on routine NCS.
Clinical Presentation
The clinical presentation is similar in primary autoimmune and secondary paraneoplastic LEMS. Fatigue is a prominent and early symptom in LEMS patients. Patients with LEMS also complain of proximal weakness, especially lower extremity weakness, sometimes mimicking a myopathy. The complaints of fatigue and proximal weakness often may seem disproportionate to the objective examination findings. When patients with suspected LEMS do not have objective detectable weakness, it may be better appreciated by watching individuals rise from a chair or climb stairs (Fig. 74-2). Muscle stretch reflexes are typically reduced or absent and this finding can be an important clue to the diagnosis. Postexercise potentiation of depressed or absent muscle stretch reflexes and of muscle strength is often demonstrable and signifies a presynaptic neuromuscular junction transmission disorder.