CHAPTER 32 Nose, nasal cavity and paranasal sinuses
The nose is the first part of the upper respiratory tract, and is responsible for warming, humidifying, and, to some extent, filtering inspired air. It also houses the olfactory epithelium which contains olfactory receptor neurones responsible for detecting airborne odorant molecules.
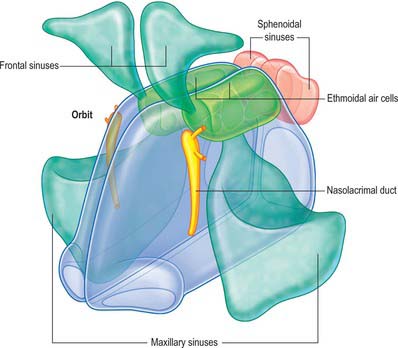
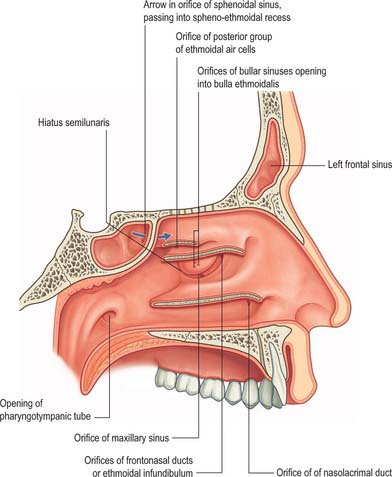
The nose may be subdivided into an external nose, which opens anteriorly onto the face through the nostrils or nares, and an internal chamber, divided sagittally by a septum into right and left cavities which open posteriorly into the nasopharynx through the posterior nasal apertures or choanae. The nasal cavities are housed in a supporting framework composed of bone and fibro-elastic cartilages. The larger bones in this framework contain air-filled spaces lined with respiratory epithelium, described collectively as the paranasal sinuses. The sinuses and the nasolacrimal ducts drain into the nasal cavity via openings in its lateral walls (Fig. 32.1).
EXTERNAL NOSE
BONE AND CARTILAGE
Bony skeleton of the external nose
The piriform aperture has sharp edges. It is bounded below and laterally by the maxilla and above by the nasal bones (Fig. 32.2). The lateral part of the inferior edge of the piriform aperture merges into its lateral wall, which is formed by the frontal process of the maxilla. It is bounded above by the nasal part of the frontal bone and superomedially by the lateral edge of the nasal bone. The bony nasal septum articulates with the undersurface of the nasal bones and provides support to the dorsum of the nose. The nasal bones vary in thickness and width, which is of significance in planning osteotomies. They are thick and widest at the nasofrontal suture, narrow at the nasofrontal angle before they widen, and become thinner 9–12 mm below the nasofrontal angle.
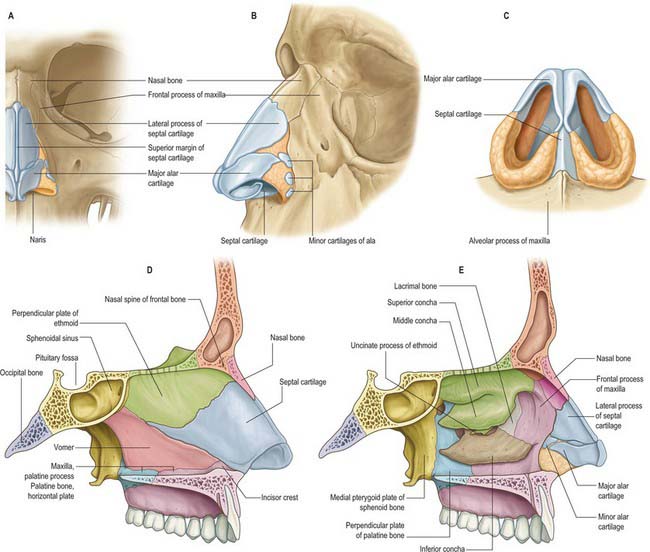
Cartilaginous skeleton of the external nose
The cartilaginous framework consists of the paired lateral and major cartilages and several minor alar nasal cartilages (Fig. 32.2).
Major alar cartilage
The major alar cartilage is a thin flexible plate. It lies below the upper lateral cartilage and curves acutely around the anterior part of its naris. The medial part, the narrow medial crus (septal process), is loosely connected by fibrous tissue to its contralateral counterpart and to the anteroinferior part of the septal cartilage. The intermediate crus forms the margin of the apex of the nostril. The lateral crus lies lateral to the naris and runs superolaterally away from the margin of the nasal ala. The upper border of the lateral crus of the major alar cartilage is attached by fibrous tissue to the lower border of the lateral nasal cartilage. Its lateral border is connected to the frontal process of the maxilla by a tough fibrous membrane containing three or four minor alar cartilages. The junction between the lateral crura of the major alar and lateral cartilages is variable: the two edges may abut or overlap, in which case the lateral crus is then the more lateral at the junction. The lateral crus of the major alar cartilage is shorter than the lateral margin of the naris and runs away from the margin of the ala nasi. The lateral part of the margin of the ala nasi is fibroadipose tissue covered by skin. In front, the angulations or ‘domes’ between the medial and lateral crurae of the major alar cartilages are separated by a notch palpable at the tip of the nose.
MUSCLES
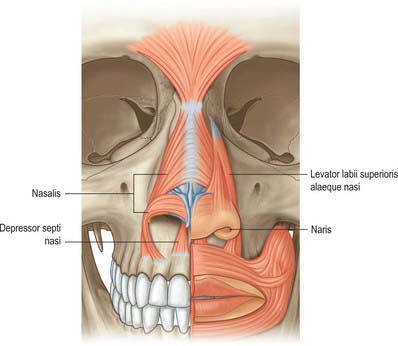
The nasal muscle group includes procerus, nasalis, dilator naris anterior, depressor septi and levator labii superioris alaequae nasi (Fig. 32.3). These muscles are involved in respiration, facial expression and in the production of some sounds during speech, when their activity is dependent upon the activity of orbicularis oris and the type of sound (see Clark et al 1998). Any or all of these muscles may be absent in cleft lip deformities with corresponding functional and aesthetic consequences.
Procerus
Procerus is a small pyramidal muscle that lies close to, and is often partially blended with, the medial side of the frontal part of occipitofrontalis. It arises from a fascial aponeurosis attached to the periosteum covering the lower part of the nasal bone, the perichondrium covering the upper part of the lateral nasal cartilage and the aponeurosis of the transverse part of nasalis. It is inserted into the glabellar skin over the lower part of the forehead between the eyebrows.
CUTANEOUS VASCULAR SUPPLY AND LYMPHATIC DRAINAGE
Nasal skin receives its blood supply from branches of the facial, ophthalmic and infraorbital arteries. The alae and lower part of the nasal septum are supplied by lateral nasal and septal branches of the facial artery and the lateral aspects and dorsum of the nose are supplied by the dorsal nasal branch of the ophthalmic artery and the infraorbital branch of the maxillary artery. The venous networks draining the external nose do not run parallel to the arteries but correspond to arteriovenous territories of the face. The frontomedian region of the face, including the nose, drains to the facial vein, and the orbitopalpebral area of the face, including the root of the nose, drains to the ophthalmic veins. The connections of the veins of the nose, upper lip and cheek with the drainage area of the ophthalmic veins are clinically significant because they can be the route which spreads infection and initiates thrombosis of the major intracranial sinuses. Lymph drainage is primarily to the submandibular group of nodes although lymph draining from the root of the nose drains to superficial parotid nodes. There is experimental evidence that nasal lymphatics might play a major role in CSF transport in animals such as the sheep: there is currently very little evidence that a similar pathway exists in humans (but see Johnston et al 2004).
NASAL CAVITY
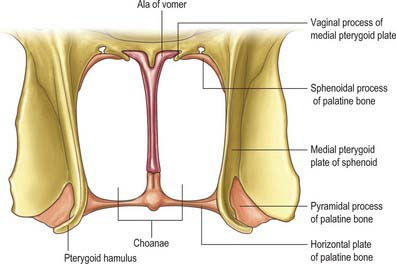
The nasal cavity communicates with the frontal, ethmoidal, maxillary and sphenoidal paranasal sinuses and opens into the nasopharynx through a pair of oval openings, the posterior nasal apertures or choanae. The latter are separated by the posterior border of the vomer, and each is limited above by the vaginal process of the medial pterygoid plates, laterally by the perpendicular plate of the palatine bone and the medial pterygoid plate, and below by the horizontal plate of the palatine bone (Fig. 32.4). The adult choana typically measures 2.5 cm in vertical height and 1.3 cm transversely: size is not usually affected by deviations of the nasal septum. The vomerovaginal and palatovaginal canals are found in the roof of this region.
Each half of the nasal cavity has a roof, floor, medial (septal) and lateral walls and a vestibule.
ROOF
The roof is horizontal in its central part and slopes downwards in front and behind (Fig. 32.3). The anterior slope is formed by the nasal spine of the frontal bones and by the nasal bones. The central region is formed by the cribriform plate of the ethmoid bone which separates the nasal cavity from the floor of the anterior cranial fossa. It contains numerous small perforations which transmit the olfactory nerves and their ensheathing meningeal layers, and a separate anterior foramen which transmits the anterior ethmoidal nerve and vessels. The posterior slope is formed by the anterior aspect of the body of the sphenoid, interrupted on each side by an opening of a sphenoidal sinus, and the sphenoidal conchae or superior conchae.
MEDIAL WALL
The medial wall of each nasal cavity is the nasal septum, a thin sheet of bone (posteriorly) and cartilage (anteriorly), that lies between the roof and floor of the cavity (Fig. 32.2D).
Bony septum
The septum is usually relatively featureless but sometimes exhibits ridges or bony spurs. The posterosuperior part of the septum and its posterior border are formed by the vomer, which extends from the body of the sphenoid to the hard palate (for more details, see Chapter 29). Its surface is grooved by the nasopalatine nerves and vessels. The anterosuperior part of the septum is formed by the perpendicular plate of the ethmoid which is continuous above with the cribriform plate. Other bones which make minor contributions to the septum at the upper and lower limits of the medial wall are the nasal bones and the nasal spine of the frontal bones (anterosuperior), the rostrum and crest of the sphenoid (posterosuperior), and the nasal crests of the maxilla and palatine bones (inferior).
Cartilaginous septum
Vomeronasal organ
In most amphibia, reptiles and mammals, the vomeronasal organ is the peripheral sensory organ of the accessory olfactory system. In these animals, paired vomeronasal organs are located either at the base of the nasal septum or in the roof of the mouth, and are involved in chemical communication that often, but not exclusively, is mediated via pheromones. In many macrosomatic animals the vomeronasal organ consists of a vomeronasal duct which contains chemosensory cells, and a vomeronasal nerve which terminates in the accessory olfactory bulb in the CNS. Whether adult humans possess a vomeronasal organ remains controversial; it is claimed that the duct sometimes persists beyond the embryonic stage (for detailed reviews, see Meredith 2001, Witt & Hummel 2006) but no neural connection appears to be present in humans after birth.
LATERAL WALL
The lateral wall of the nasal cavity is formed anteroinferiorly by the maxilla and its anterior and posterior fontanelles (bony deficiencies in the medial wall of the maxilla which are obliterated to varying degrees by fibrous tissue); posteriorly by the perpendicular plate of the palatine bone; and superiorly by the labyrinth of the ethmoid bone. It contains three projections of variable size, the inferior, middle and superior nasal conchae (turbinates) (Figs 32.2E, 32.5). The conchae curve generally inferomedially, each roofing a groove, or meatus, which is open to the nasal cavity. The middle conchae may also curve inferolaterally, or may be expanded by an enclosed air cell to form a so called ‘concha bullosa’ (30% of individuals) or have a concave medial surface, known as a paradoxical turbinate (10% of individuals).
Inferior concha and inferior meatus
The inferior concha is a thin, curved, independent bone (for more details, see Chapter 29). It articulates with the nasal surface of the maxilla and the perpendicular plate of the palatine bone. Its free lower border is gently curved and the subjacent inferior meatus reaches the nasal floor. The inferior meatus is the largest meatus, and it extends along almost all of the lateral nasal wall. It is deepest at the junction of its anterior and middle thirds, where it admits the inferior opening of the nasolacrimal canal (see Ch. 39). The canal is formed by the articulations between the lacrimal groove of the maxilla, the descending process of the lacrimal bone and the lacrimal process of the inferior concha. During postnatal development, the ostium of the nasolacrimal duct moves upwards and is increasingly hidden under the over-arching inferior concha.
Middle concha and middle meatus
The middle concha is a medial process of the ethmoidal labyrinth and may be pneumatized (conchal sinus). It extends back to articulate with the perpendicular plate of the palatine bone. The region beneath it is the middle meatus, which is deeper in front than behind, lies below and lateral to the middle concha, and continues anteriorly into a shallow fossa above the vestibule, termed the atrium of the middle meatus.






