“Macrocystic” pattern: Few (< 6) macrocystic locules, which are relatively large (> 2 cm)
Usually of simple fluid attenuation, but may be mildly hyperdense due to hemorrhage or protein
Frequent peripheral curvilinear calcifications or calcifications in septations (16% of cases)
Presence of thick wall, mural nodularity, or thick septations suggests invasive malignancy
No apparent communication with main pancreatic duct
• MR: Usually simple fluid signal (high T2; low T1), but may be slightly less T2 hyperintense due to mucin content
Internal septations (which are T2 hypointense) easier to perceive on MRI compared to CT
MRCP: No communication with main pancreatic duct
PATHOLOGY
• Tumor shares clinical and pathologic characteristics of biliary tumors, ovarian tumors, and IPMN
• Presence of ovarian stroma lining cyst is key feature for diagnosis of mucinous cystic neoplasm (MCN)
CLINICAL ISSUES
• Strong preponderance in middle-aged women (99%)
• Considered premalignant or frankly malignant: Rate of malignancy in different series ranges between 10-40%
• Risk factors for invasive malignancy: Older age, lesion size, mural nodularity, thick wall, patient symptoms (pain, pancreatitis), and ↑ CEA and CA 19-9
• MCNs typically undergo complete surgical resection with adjuvant chemotherapy for malignant lesions
• Malignant MCNs receive adjuvant chemotherapy after surgical resection
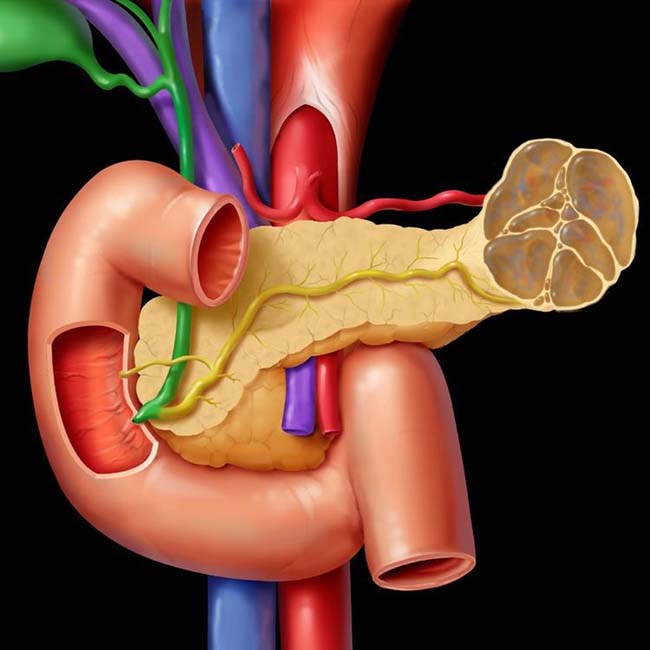
(Left) Graphic of a mucinous cystic tumor shows a multiseptate, mucin-filled, cystic mass in the pancreatic tail that displaces the pancreatic duct.
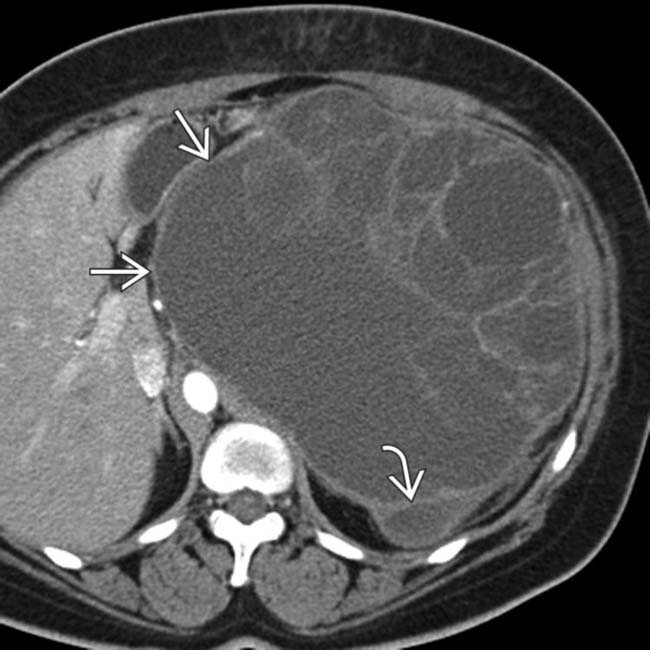
(Right) Axial CECT in a 35-year-old woman demonstrates a large complex cystic mass arising from the pancreatic tail with multiple internal cystic locules and septations, some of which are thick . This mass was found to be a mucinous cystic neoplasm (MCN) with invasive adenocarcinoma at surgery.
(Left) Axial CECT in a 46-year-old woman demonstrates a large, simple-appearing cyst arising from the upstream pancreatic body.
(Right) Axial T2 FS MR in the same patient confirms the lack of complexity within the T2-hyperintense cyst . MR can sometimes show complexity and suspicious features that might be difficult to identify on CT. This was found to be a MCN with low-grade dysplasia at surgery.
TERMINOLOGY
Synonyms
• Mucinous cystic neoplasm (MCN), mucinous macrocystic neoplasm or adenoma, mucinous cystadenoma or cystadenocarcinoma
Definitions
• Thick-walled, unilocular or multilocular pancreatic tumor composed of large, mucin-containing cysts
Some sources suggest presence of ovarian stroma within lesion is necessary for diagnosis
• MCN and intraductal papillary mucinous neoplasm (IPMN) are together classified as pancreatic mucinous tumors
IMAGING
General Features
• Best diagnostic clue
Large, unilocular or multilocular encapsulated cystic mass with septations and thick wall in pancreatic tail
• Location
Tail of pancreas (more common)
Presents as single lesion (not multifocal like IPMN)
• Size
2-12 cm in diameter
– MCNs usually larger than serous cystadenoma or IPMN
Size is predictor of biologic behavior
– Lesions < 40 mm found to have low risk of malignancy in recent series
• Morphology
Typically round/ovoid, but may be ill defined/irregular
Radiographic Findings
• ERCP
Displacement and narrowing of main pancreatic duct adjacent to tumor
Can differentiate IPMN (which communicate with main pancreatic duct) from MCN (which do not communicate)
CT Findings
• Unilocular or multilocular encapsulated cyst in pancreatic body/tail with frequent internal septations
“Macrocystic” pattern: Few (< 6) macrocystic locules that are relatively large (> 2 cm)
• Usually of simple fluid attenuation, but may be mildly hyperdense due to hemorrhage or protein
• Frequent peripheral curvilinear calcifications or calcifications in septations (16% of cases)
• Presence of thick, irregular wall, internal mural nodularity, or thick septations suggest invasive malignancy
Upstream pancreatic ductal dilatation or atrophy suggest invasive malignancy
• No apparent communication with main pancreatic duct
In rare instances, some series have suggested possible communication with pancreatic duct in very small minority of lesions
MR Findings
• Typically show simple fluid signal (high T2; low T1), but may be slightly less T2 hyperintense due to mucin content
May show areas of T1 hyperintensity due to internal hemorrhage, proteinaceous content, or mucin
• Internal septations (typically T2 hypointense) easier to perceive on MR compared to CT
• Calcifications often not visible on MR: If visible, are low signal on all pulse sequences
• Thick, enhancing septations, wall thickening, and mural nodularity on T1WI C+ suggest invasive malignancy
• MRCP: No communication with pancreatic duct
• DWI: No role in differentiating mucinous from nonmucinous lesions or benign from malignant
Ultrasonographic Findings
• Grayscale ultrasound
Multiloculated cystic mass with echogenic internal septa
– Often associated with thick wall ± mural nodularity
Can also appear as unilocular anechoic mass
Angiographic Findings
• Conventional
Predominantly avascular mass
Cyst wall and solid component
– Show small areas of vascular blush and neovascularity
Displacement of surrounding arteries and veins by cysts
Imaging Recommendations
• CECT or MR
DIFFERENTIAL DIAGNOSIS
Pancreatic Pseudocyst
• Usually known history of pancreatitis or alcoholism ± imaging stigmata of chronic pancreatitis (pancreatic calcifications, ductal beading, etc.)
• Loculated cyst with adjacent peripancreatic fat stranding/inflammation
• Evolves over time from acute peripancreatic fluid collection into loculated pseudocyst
• Communication with pancreatic duct is frequent (70% of cases) and may be visible on ERCP or MRCP
• Lab data: Increased amylase in cyst and serum
• When occurring in pancreatic tail, may simulate unilocular mucinous cystic neoplasm
Pancreatic Serous Cystadenoma
• Well-circumscribed, lobulated cystic mass most often occurring in pancreatic head
• Classic appearance (“microcystic” or “sponge” lesion): Many small cysts separated by thin septa and with central scar demonstrating calcification
Calcification more common in serous than mucinous pancreatic neoplasms (38% vs. 16%)
• Macrocystic, oligocystic, and unilocular variants of serous cystadenoma difficult to distinguish from MCN
Thick wall and mural nodularity unusual with serous cystadenoma
Pancreatic IPMN
• Mucin-producing neoplasms which are classified into 3 types with different risks of malignancy
Side-branch IPMN: Arise in pancreatic duct side branch and carry risk of invasive malignancy of 17%
Main pancreatic duct (MPD): Arise in main pancreatic duct and carry high risk of malignancy (58%)
Combined type IPMN: Features of both side branch and main duct IPMN with prognosis similar to main duct IPMN
• Side-branch or combined type IPMN: Cyst (± nodularity, septations, calcifications) that communicates with pancreatic duct
Cystic Pancreatic Neuroendocrine Tumor
• Cystic neuroendocrine tumors more likely to be non-insulin producing and nonsyndromic
• Cystic lesion without pancreatic ductal dilatation or atrophy
Differentiate from IPMN/MCN by presence of peripheral hyperenhancement on arterial phase CECT or MR
Buy Membership for Radiology Category to continue reading. Learn more here






 arising from the pancreatic tail with multiple internal cystic locules and septations, some of which are thick
arising from the pancreatic tail with multiple internal cystic locules and septations, some of which are thick  . This mass was found to be a mucinous cystic neoplasm (MCN) with invasive adenocarcinoma at surgery.
. This mass was found to be a mucinous cystic neoplasm (MCN) with invasive adenocarcinoma at surgery.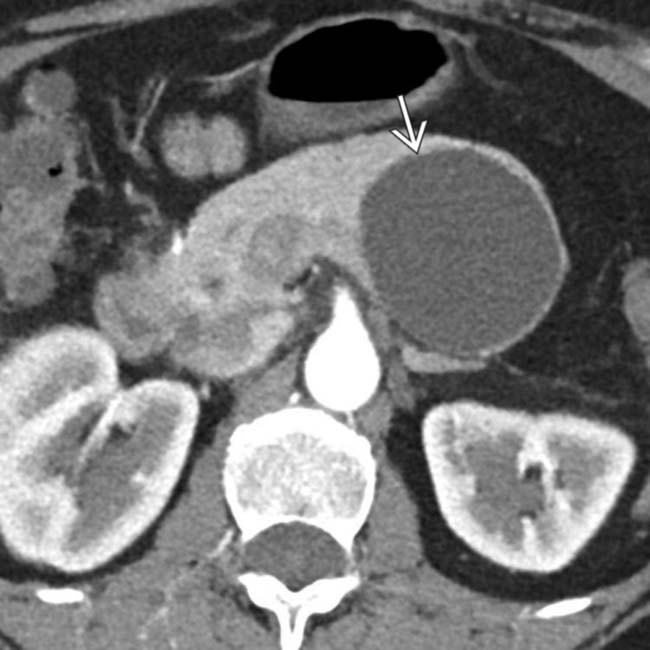
 arising from the upstream pancreatic body.
arising from the upstream pancreatic body.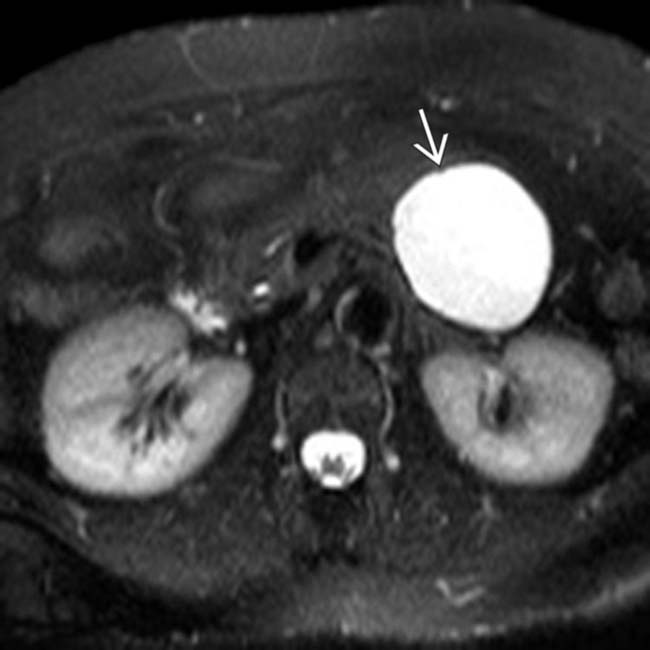
 . MR can sometimes show complexity and suspicious features that might be difficult to identify on CT. This was found to be a MCN with low-grade dysplasia at surgery.
. MR can sometimes show complexity and suspicious features that might be difficult to identify on CT. This was found to be a MCN with low-grade dysplasia at surgery.


























