Chapter 225 Management of Traumatic Unilateral Jumped Cervical Facet Joint without Myelopathy
Closed Traction Reduction Then Surgery
Description and Mechanism
The most common activities associated with this type of injury include motor vehicle accidents, falls, and sports injuries. These injuries typically occur in the cervical spine due to the anatomy of the facet joints, which allow them to be very mobile. The mechanism of these injuries has been attributed to combined flexion and rotation. Some authors have postulated that the unilateral facet dislocation is mainly due to a flexion load with a rotational component.1–3 The rotational component of the injury is often evident on plain radiographs, with the superior segment of the spine rotated. The patient often appears to be looking to the side. The diagnostic accuracy is enhanced by a review of the anteroposterior projection on plain radiographs of the cervical spine. These often reveal malalignment or offset of the spinous processes. Unilateral cervical facet dislocation and fracture-dislocations of the cervical spine are relatively uncommon injuries that can result in spinal cord or nerve root injury. They represent approximately 12% to 16% of all cervical spine injuries.4 The goal of treatment is to prevent further injury, attempt to restore normal neurologic function, and reduce axial and radicular pain.
Diagnosis
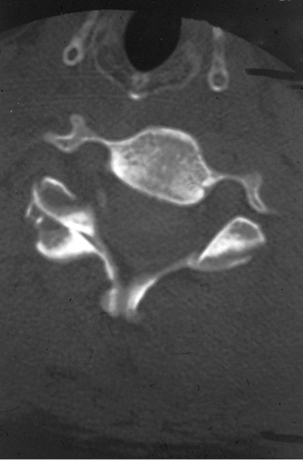
Plain radiographs demonstrate a characteristic appearance on the lateral radiograph, demonstrating anterolisthesis of the upper vertebra, usually measuring less than 25% of the anteroposterior dimension of the body (Fig. 225-1). This differs from bilateral facet dislocations, in which there commonly is a 50% subluxation (Fig. 225-2). On the anteroposterior view, the spinous processes above the level of the injury rotate to the same side as the dislocated facet. On the lateral radiograph, instead of the facets being in a superimposed position, they are seen individually and separately at the level of the injury. This creates the so-called bow-tie sign seen on CT. The lateral radiograph may also show increased distance between adjacent spinous processes at the level of the injury, which may be due to a disruption in the dorsal ligamentous complex. Oblique radiographs may reveal obstruction of the neuroforamen by the dislocated facet. A CT scan may reveal that the articular surface of the facet is observed to be without the appropriate articulating mate or that the appropriate articulating mate may be on the wrong side of the facet (the so-called naked facet sign or reversed hamburger bun sign) (Fig. 225-3).


Treatment
The primary goal in the treatment of this injury is to prevent further damage to the spinal cord and neural elements. The secondary goal is to relieve neural compression. This may be achieved by directly decompressing and removing the compressing elements or restoring the normal alignment of the cervical spine with distraction. The treatment of this injury with cervical traction was popularized by Crutchfield. It now includes attempted awake closed reduction with Gardner-Wells tongs5,6 (Fig. 225-4). The use of cervical traction is also referred to as closed reduction, because a skin incision is not made. Once the spine is aligned with a closed reduction, there remains a need to fuse the unstable segments, which requires an open procedure. Fixation and fusion can be performed either through an anterior or posterior approach.7 If closed reduction fails, open reduction may be achieved via either an anterior or posterior approach, followed by fixation and fusion.8–11 A preoperative MRI can provide information about the presence of a disc herniation and spinal cord compression. If disc herniation is present, a ventral decompression should be considered to decompress the spinal cord before manipulation. In addition, the spinal column can be manipulated and reduced through a ventral approach.

The initial weight used for traction should not be greater than 10 pounds (4.6 kg) to avoid overdistraction at the level of injury. The weight may be increased by 5- to 10-pound (2.3–4.6 kg) increments, usually at 10- to 15-minute intervals, until the desired alignment is achieved. It is important that with each increase in the traction weights, the patient is examined both neurologically and with plain radiographs. Under most circumstances, the total weight should not exceed 10 pounds per vertebral level. Gentle manual torsion toward the side of the jumped facets (straightening the head) may also aid reduction. In addition the use of paraspinal muscle relaxation using IV diazepam and/or narcotics may provide an easier reduction. The downside to muscle relaxants and narcotics is that they may mask results of the neurologic examination and as such should be used judiciously.
An initial attempt at closed reduction using skeletal traction is not without risk. The most serious complication of cervical traction and closed reduction is the retropulsion of disc fragments into the spinal canal and resultant spinal cord compression. Several reports of neurologic deterioration after closed reduction in the setting of concurrent disc herniation have been described.12 This deterioration, however, is rare and a permanent major neurologic deficit has not been documented with closed reduction in an awake, alert patient without distraction injuries. The aforementioned has led to a debate as to whether MRI should be obtained before closed reduction of dislocated facets.13 In addition, late instability is relatively common in patients treated with closed reduction alone without arthrodesis because of the concomitant presence of significant ligamentous disruption associated with these injuries. When traction is sufficient, the facets are usually distracted or perched and they reduce spontaneously.
The natural history of most spinal cord injuries after a unilateral jumped facet seems to consist of some improvement, with or without reduction—typically in the form of return of the impaired nerve root at the level of the injury or the next caudal level. In the past, controversy surrounding the best method of obtaining and maintaining reduction of unilateral facet dislocation was commonplace. Bohler,14 Crutchfield,15 and Ramadier and Bombart16 recommended that a patient with such an injury be treated with skull-tong traction, with progressively increased weights to obtain reduction. Failure of this procedure to achieve reduction was considered an indication for open reduction and posterior cervical fusion by Bohlman,9,10 Jacobs,11 and Bailey.8 In the past, Galibert,17 Evans,18 and Burke and Berryman19 described considerable success with gentle head and neck manipulation under general anesthesia in patients with unilateral facet dislocation. Bailey8 and Durbin20





