Kidney Clinical Assessment and Diagnostic Procedures
History
The history begins with a description of the chief complaint, stated in the patient’s own words. A description of the chief complaint includes the onset, location, duration, and factors or strategies that lessen or aggravate the problem.1 The individual should be encouraged to describe the effects of any treatment for the problem, prescription and nonprescription medications taken to alleviate symptoms, efforts taken to determine the cause of the problem, and procedures performed to improve the problem. A careful history that explores symptoms fully is an essential component of the clinical assessment.
Predisposing factors for acute kidney dysfunction are obtained during the history, including the use of over-the-counter medicines, recent infections requiring antibiotic therapy, antihypertensive medicines, and any diagnostic procedures performed using radiopaque contrast.2 Nonsteroidal anti-inflammatory medications (e.g., ibuprofen), antibiotics (especially aminoglycosides), antihypertensives (especially medicines that block angiotensin),3 and iodine-based dyes may cause an acute or chronic decline in kidney function. A history of recent onset of nausea and vomiting or appetite loss caused by taste changes (uremia often causes a metallic taste) may provide clues to the rapid onset of kidney problems.2 Symptoms that indicate rapid fluid volume gains are explored. For example, weight gains of more than 2 pounds per day, sleeping on additional pillows, and sitting in a chair to sleep are signals of volume overload and potential cardiac stress related to kidney dysfunction.
The family history may provide important information that points to the kidneys as the source of the patient’s symptoms. For example, the patient may reveal that one or two close family members have always had swelling of the extremities or high blood pressure. These symptoms should lead to questions about a history of kidney problems in the family. Box 26-1 summarizes the information gained from a kidney history.
Physical Examination
Inspection
Bleeding
Visual inspection related to the kidneys focuses on the patient’s flank and abdomen. Kidney trauma is suspected if a purplish discoloration is present on the flank (Grey-Turner sign) or near the posterior 11th or 12th ribs.1 Bruising, abdominal distention, and abdominal guarding may also signal kidney trauma or a hematoma around a kidney. Individuals who have experienced a traumatic injury should be carefully assessed for signs of kidney trauma.
Volume
Inspection is especially helpful in looking for signs of volume depletion or overload that may signal or lead to kidney problems. Fluid volume assessment begins with an inspection of the patient’s jugular neck veins. The supine position facilitates normal jugular venous distention. An absence of distention (flat neck veins) indicates hypovolemia. Assessment continues with the head of the bed elevated 45 to 90 degrees.1 Fluid overload exists when the neck veins remain distended more than 2 cm above the sternal notch when the bed is at 45 degrees.4
Assessment of skin turgor provides additional data for identifying fluid-related problems. To assess turgor, the skin over the forearm is picked up and released.5 Normal elasticity and fluid status allow an almost immediate return to shape after the skin is released. In fluid volume deficit, however, the skin remains raised and does not return to its normal position for several seconds.5 Because of the loss of skin elasticity in older persons, skin turgor assessment may not be as accurate a fluid assessment measure for this age group.
Inspection of the oral cavity provides clues to fluid volume status. When a fluid volume deficit exists, the mucous membranes of the mouth become dry. However, mouth breathing and some medicines (e.g., antihistamines) can also dry the mucous membranes temporarily. The most accurate way to assess the oral cavity is to inspect the mouth using a tongue blade and light. Dryness of the oral cavity is more indicative of fluid volume deficit than are complaints of a dry mouth.4
Edema
Edema can be assessed by applying fingertip pressure on the swollen area over a bony prominence, such as the ankles, pretibial areas (shins), and sacrum. If the indentation made by the fingertip does not disappear within 15 seconds, pitting edema exists. Pitting edema indicates increased interstitial volume, and it usually is not evident until significant weight gain has occurred. Edema also may appear in the hands and feet, around the eyes, and in the cheeks. Dependent areas, such as the feet and sacrum, are the areas most likely to demonstrate edema in patients confined to a wheelchair or bed. One way of measuring the extent of edema is by using a subjective scale of 1 to 4, with 1 indicating only minimal pitting and 4 indicating severe pitting (Table 26-1).1 Other scales for assessing and measuring edema can be used (see Table 13-3).
TABLE 26-1
| RATING | APPROXIMATE EQUIVALENT |
| +1 | 2-mm depth |
| +2 | 4-mm depth (lasting up to 15 sec) |
| +3 | 6-mm depth (lasting up to 60 sec) |
| +4 | 8-mm depth (lasting longer than 60 sec) |
Auscultation
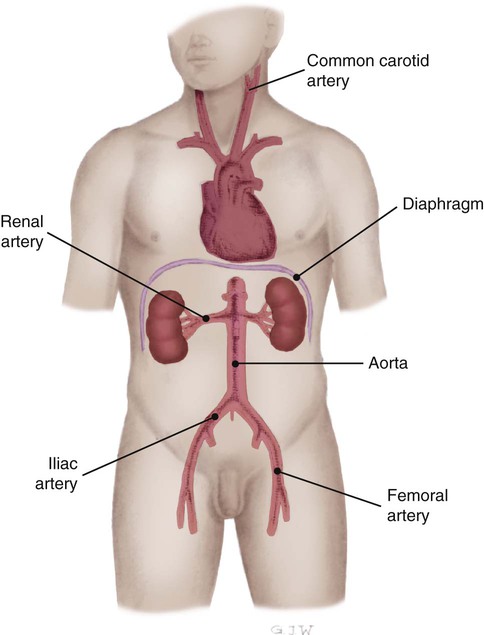
Auscultation of the kidneys yields virtually no useful information. However, the renal arteries are auscultated for a bruit, a blowing or swishing sound that resembles a cardiac murmur (Fig. 26-1). The examiner listens for bruits above and to the left and right of the umbilicus.1 A renal artery bruit usually indicates stenosis, which may lead to acute or chronic kidney dysfunction due to compromised blood flow to one or both kidneys. A bruit over the upper portion of the abdominal aorta may indicate an aneurysm or a stenotic area that can decrease blood flow to the kidneys.
Heart
Auscultation of the heart requires assessing the rate and rhythm and listening for extra sounds. Fluid overload is often accompanied by a third or fourth heart sound, which is best heard with the bell of the stethoscope.1 Increased heart rate alone provides little information about fluid volume, but combined with a low blood pressure, it may indicate hypovolemia.
The heart is auscultated for the presence of a pericardial friction rub. A rub can best be heard at the third intercostal space to the left of the sternal border while the individual leans slightly forward.1 A pericardial friction rub indicates pericarditis, and it may result from uremia in a patient with kidney failure.
Blood Pressure
Blood pressure and heart rate changes are very useful in assessing fluid volume deficit.3 In stable critically ill patients or in patients on a telemetry unit, orthostatic vital sign measurements provide clues to blood loss, dehydration, unexplained syncope, and the effects of some antihypertensive medications. A drop in systolic blood pressure of 20 mm Hg or more, a drop in diastolic blood pressure of 10 mm Hg or more, or a rise in pulse rate of more than 15 beats/min from lying to sitting or from sitting to standing indicates orthostatic hypotension. Box 26-2 describes how to assess for orthostatic hypotension. The drop in blood pressure occurs because a sufficient preload is not immediately available when the patient changes position. The heart rate increases in an attempt to maintain cardiac output and circulation. Orthostatic hypotension produces subjective feelings of weakness, dizziness, or faintness. Orthostatic hypotension occurs with hypovolemia, prolonged bed rest, or as a side effect of medications that affect blood volume or blood pressure.
Palpation
Although rarely performed in critically ill patients, palpation of the kidneys in stable patients provides information about the kidneys’ size and shape. Palpation of the kidneys is achieved through the bimanual capturing approach. Capturing is accomplished by placing one hand posteriorly under the flank of the supine patient with the examiner’s fingers pointing to the midline and placing the opposite hand just below the rib cage anteriorly.1,2 The patient is asked to inhale deeply while pressure is exerted to bring the hands together (Fig. 26-2). As the patient exhales, the examiner may feel the kidney between the hands. After each kidney is palpated in this manner, the two should be compared for size and shape. Each kidney should be firm and smooth, and the two organs should be of equal size. The examiner is usually unable to palpate a normal left kidney. The right kidney is more easily palpated because of its lower position, caused by downward displacement by the liver. Problems should be suspected if a mass (cancer) or an irregular surface (polycystic kidneys) is palpated, a size difference is detected, the kidney extends significantly lower than the rib cage on either side, or there is evidence of recent blunt trauma.1

Percussion
Kidneys
Percussion of a kidney is performed with the patient in a side-lying or sitting position, with the examiner’s hand placed over the costovertebral angle (lower border of the rib cage on the flank).1 Striking the back of the hand with the opposite fist produces a dull thud, which is normal. Pain may indicate infection (e.g., urinary tract infection that has extended into the kidneys) or injury resulting from trauma. Traumatic injury to the kidneys should be assessed in the presence of a penetrating abdominal wound, with blunt abdominal trauma, or with a fractured pelvis or ribs.
Abdomen
Observation and percussion of the abdomen may help in assessing fluid status. Percussing the abdomen with the patient in the supine position generally yields a dull sound (solid bowel contents or fluid) or a hollow sound (gaseous bowel).1
Ascites, or excess fluid accumulation and distention of the abdominal cavity, is an important observation in determining fluid overload. Differentiating ascites from distortion caused by solid bowel contents is accomplished by producing a fluid wave. A fluid wave is elicited by exerting pressure to the abdominal midline while one hand is placed on the right or left flank.1 Tapping the opposite flank produces a wave in the accumulated fluid that can be felt under the hands (Fig. 26-3). Other signs of ascites include a protuberant, rounded abdomen and abdominal striae.1

Additional Assessments
Weight Monitoring
Whenever possible, the patient is weighed during admission to the critical care unit. It is important to document whether the current weight differs significantly from the weight 1 to 2 weeks before admission to the hospital. The patient is weighed daily for comparison with the previous day’s weight. The weight is obtained at the same time each day, with the patient wearing the same amount of clothing and using the same scales. The individual’s weight is of critical importance to the dialysis nurse caring for a patient with acute or chronic kidney failure. The differences in weight from day to day are used to calculate the amount of fluid to remove during a dialysis treatment.6
Intake and Output Monitoring
Individuals with acute kidney injury (AKI) often exhibit a decrease in urine output, or oliguria (less than 0.5 mL/kg/hr in adults; less than 1 mL/kg/hr in infants and young children). However, there may be a fairly normal or only slightly decreased urine output that reflects water removal without solute removal in the early phases of AKI. Although urine output is a sensitive indicator, kidney function cannot be accurately determined by urine output alone. For additional information on AKI see Chapter 27.
Hemodynamic Monitoring
Body fluid status is accurately reflected in measurements of cardiovascular hemodynamics. Measurements such as central venous pressure (CVP), pulmonary artery occlusion pressure (PAOP), cardiac index (CI), and mean arterial pressure (MAP) provide a clear picture of the increases or decreases in vascular volume returning to and being ejected from the heart.7 Volume depletion and volume overload are easily detected by use of central venous or arterial catheters, from which pressure measurements can be obtained (Table 26-2).
TABLE 26-2
HEMODYNAMIC ASSESSMENT OF FLUID STATUS
| MEASUREMENT | VOLUME DEPLETION | VOLUME OVERLOAD |
| Central venous pressure (CVP) | <2 mm Hg | >5 mm Hg |
| Pulmonary artery occlusion pressure (PAOP) | <5 mm Hg | >12 mm Hg |
| Cardiac index (CI) | <2.2 L/min/m2 | >4 L/min/m2 |



