CHAPTER 34 Indications for surgery
Introduction
Glaucoma is the leading cause of irreversible blindness worldwide, affecting an estimated 60 million people in 20101. More than 50% of sufferers in developed countries are unaware of their condition and this figure increases to over 90% in the developing world. The economic burden is substantial at almost $3 billion in the US in 20042. A recent estimate of the risk of progressing to blindness in patients with diagnosed glaucoma attending a specialist glaucoma clinic in the US is around 14% for unilateral blindness and 6% for bilateral blindness after 15 years3.
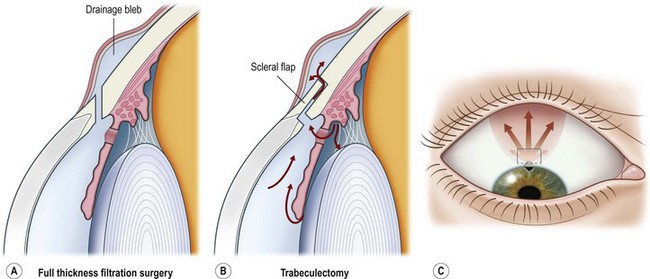
Surgery for primary open angle glaucoma (POAG) has evolved in the past 50 years from full-thickness filtration surgery, in which a hole in the scleral wall at the corneo-scleral limbus drained aqueous from the anterior chamber to a subconjunctival ‘drainage bleb’. As this procedure carried a high risk of ocular hypotony, and bleb-related endophthalmitis4,5, it evolved to a partial-thickness scleral flap which provided an extra flow resistor (Fig. 34.1)6, prevented hypotony, and consequently lowered aqueous pressure within the subconjunctival drainage bleb lowering the risk of conjunctival breakdown and infection.
As a guarded filtration procedure, trabeculectomy was safer than the full-thickness procedure. However, as satisfactory long-term IOP control could not be achieved in a significant proportion of patients, pharmacological enhancement with anti-proliferative agents (e.g. 5-fluorouracil (5FU)7 and later, mitomycin C (MMC)) was introduced in the late 1980s. While these improved success rates some safety concerns, previously reduced by the evolution of trabeculectomy from full-thickness filtration surgery, reappeared8,9. The main concerns are hypotony10 and infection, especially as trabeculectomy-related infection has a predilection for more aggressive organisms than do other types of intraocular infections11. The alteration in conjunctival surface healing that resulted from the use of 5FU, and especially MMC, also resulted in prominent drainage blebs that could cause chronic discomfort or dysesthesia12. These and a higher incidence of cataract after trabeculectomy have promoted further evolution in glaucoma surgical techniques in four main directions.
General considerations
Medical versus surgical treatment
While medical and laser treatment are usually the first lines of therapy, there are some situations where early surgery is advisable. Surgery is the principal treatment for angle closure, developmental glaucomas, and a number of secondary glaucomas. Surgery is recommended for POAG in three circumstances (Box 34.1):