Chapter 6 Hip and Thigh Ultrasound
 Additional videos for this topic are available online at www.expertconsult.com.
Additional videos for this topic are available online at www.expertconsult.com.
Hip and Thigh Anatomy
The hip joint is a synovial articulation between the acetabulum of the pelvis and the proximal femur. The joint recess extends from the acetabulum over the femur to the level of the intertrochanteric line, just beyond the femoral neck. The joint capsule becomes thickened from the iliofemoral, ischiofemoral, and pubofemoral ligaments (Fig. 6-1A) and a reflection of the joint capsule extends proximally along the femoral neck.1 The femoral head is covered by hyaline cartilage, whereas the acetabulum is lined by hyaline cartilage in an inverted U shape with a fibrocartilage labrum attached to the acetabular rim.
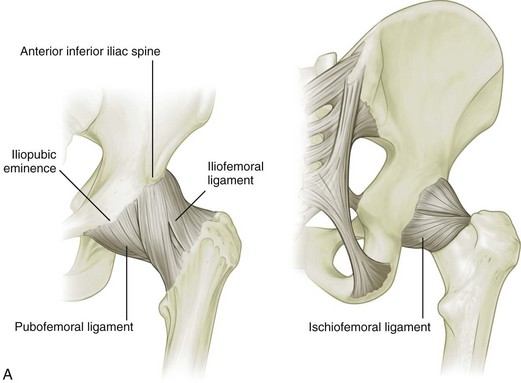
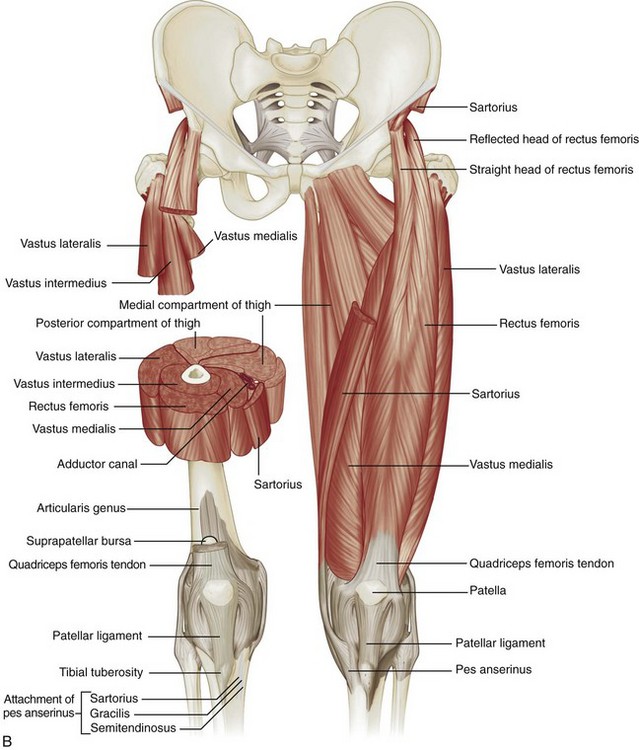
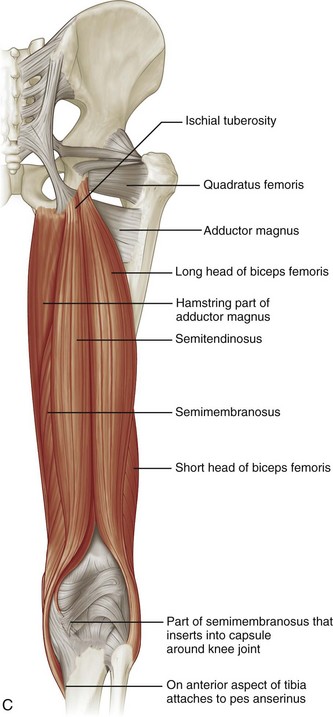
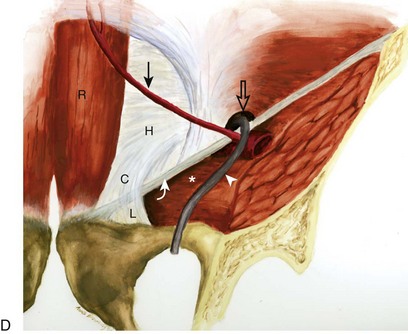
FIGURE 6-1 Hip and thigh anatomy.
(A to C, From Drake R, Vogl W, Mitchell A: Gray’s anatomy for students, Philadelphia, 2005, Churchill Livingstone; D, from Jamadar DA, Jacobson JA, Morag Y, et al: Sonography of inguinal region hernias. AJR Am J Roentgenol 187:185–190, 2006.)
Several muscles originate from the pelvis and extend across the hip joint, and others originate from the femur itself (see Fig. 6-1B and C). Muscles that originate from the posterior surface of the ilium are the gluteus minimus (which inserts on the anterior facet of the greater trochanter), the gluteus medius (which inserts on the lateral and superoposterior facets of the greater trochanter), and the gluteus maximus (which inserts on the posterior femur gluteal tuberosity below the trochanters and iliotibial tract).2 Posteriorly, the piriformis originates from the sacrum and extends inferior and lateral to insert onto the greater trochanter. Other muscles inferior to the piriformis that extend from the ischium to the proximal femur include the superior gemellus, obturator internus, inferior gemellus, and quadratus femoris.
At the anterior aspect of the hip joint, the iliopsoas can be seen as a continuation of the iliacus and psoas muscles, which inserts on the lesser trochanter. Other anterior muscles include the sartorius (which originates from the anterior superior iliac spine of the pelvis and inserts on the medial aspect of the proximal tibia) and the tensor fasciae latae (which originates from the posterolateral aspect of the ilium and inserts on the iliotibial tract, which, in turn, inserts on the proximal tibia). The rectus femoris has two origins: a direct or straight head, which originates from the anterior inferior iliac spine; and an indirect or reflected head, which originates inferior and posterior to the anterior inferior iliac spine from the superior acetabular ridge.3 Distally, the direct tendon forms an anterior superficial tendon with unipennate architecture, whereas the indirect tendon forms the central tendon with bipennate architecture.4 The rectus femoris distally combines with the vastus medialis, vastus lateralis, and vastus intermedius musculature (which all originate from the femur) to form the quadriceps tendon, which inserts on the patella and, to a lesser extent, the tibial tuberosity by way of the patellar tendon.
Medially, the adductor musculature includes the adductor longus, the adductor brevis, and the adductor magnus, which originate from the ischium and pubis of the pelvis and insert on the femur at the linea aspera and, in the case of the adductor magnus, the adductor tubercle as well. Superficial and medial to the adductors, the gracilis muscle extends from the inferior pubic ramus to the proximal tibia as part of the pes anserinus. From medially to laterally, the posterior thigh consists of the semimembranosus, the semitendinosus (both of which originate from the ischial tuberosity and insert on the proximal tibia, with the semitendinosus being part of the pes anserinus), and the biceps femoris (with long head origin from the ischial tuberosity and short head origin from the femur; the biceps femoris inserts on the fibula and lateral tibial condyle). Proximally, the semimembranosus tendon is located anterior to the conjoint tendon of the biceps femoris long head and semitendinosus and the semitendinosus muscle belly; the semimembranosus origin on the ischium is anterolateral to the conjoint tendon origin.5
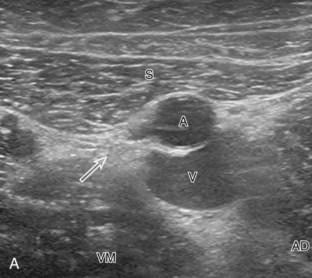
Other important structures of the anterior thigh include (medial to lateral) the femoral nerve, artery, and vein (use the mnemonic NAVEL for nerve, artery, vein, empty space, lymphatic). The sciatic nerve is seen posteriorly adjacent to the biceps femoris muscle, where it bifurcates as the tibial nerve and the common peroneal nerve laterally. Several bursae are located around the hip joint. The iliopsoas bursa is located anteriorly along the medial aspect of the iliopsoas tendon, has a convex lateral shape, and normally communicates with the hip joint in up to 15% of the population.6 The trochanteric (or subgluteus maximus) bursa is located posterolateral over the posterior and lateral facets of the greater trochanter deep to the gluteus maximus and iliotibial tract, whereas smaller subgluteus medius and subgluteus minimus bursae are located between the lateral facet and gluteus medius and the anterior facet and gluteus minimus, respectively.2 Other possible bursae include the obturator externus bursa, located medially and inferior to the femoral neck, which may communicate with the posteroinferior hip joint.7
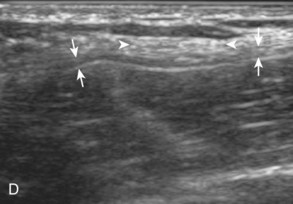
In the inguinal region, the inguinal canal represents a triangular, elongated passage in the lower abdominal wall located just superior to the inguinal ligament (see Fig. 6-1D). The inguinal canal’s posterior opening, the deep inguinal ring, is located laterally, whereas the anterior opening, called the superficial inguinal ring, is located medially near the pubis. The contents of the inguinal canal include the ilioinguinal nerve and the spermatic cord in males and the round ligament in females. The deep inguinal ring is located just lateral to the origin of the inferior epigastric artery from the external iliac artery. The inguinal (or Hesselbach) triangle is demarcated by the lateral margin of the rectus abdominis medially, the inguinal ligament inferiorly, and the superior epigastric artery laterally.8 Another structure near the inguinal ligament is the lateral femoral cutaneous nerve. This peripheral nerve exits the pelvis to extend over the lateral thigh in a somewhat variable manner—it may course across the iliac crest, within the sartorius tendon, within the inguinal ligament, or under the inguinal ligament.9 The lateral femoral cutaneous nerve may also branch proximal to the inguinal ligament.
Ultrasound Examination Technique
Table 6-1 is a checklist for hip and thigh ultrasound examination. Examples of diagnostic hip ultrasound reports are available online at www.expertconsult.com (see eBox 6-1 and 6-2).
| Location | Structures of Interest |
|---|---|
| Hip: anterior | Hip joint, iliopsoas, rectus femoris, sartorius, pubic symphysis |
| Hip: lateral | Greater trochanter, bursae |
| Hip: posterior | Sacroiliac joints, piriformis, hip abductors |
| Inguinal region | Deep inguinal ring, Hesselbach triangle, femoral artery region |
| Thigh: anterior | Rectus femoris, vastus medialis, vastus intermedius, vastus lateralis |
| Thigh: medial | Femoral artery and nerve, sartorius, gracilis, adductors |
| Thigh: posterior | Semimembranosus, semitendinosus, biceps femoris, sciatic nerve |
eBox 6-1 Sample Diagnostic Hip Ultrasound Report
Normal
Examination: Ultrasound of the Right Hip
History: Hip pain, evaluate for bursitis
Findings: The hip joint is normal without effusion or synovial hypertrophy. Limited evaluation of the anterior labrum is unremarkable. No evidence of iliopsoas bursal distention or snapping iliopsoas tendon with dynamic imaging. The remaining anterior tendons, including the rectus femoris and sartorius, as well as the adductors, are normal.
Evaluation of the lateral hip is normal. No evidence of abnormal bursal distention around the greater trochanter. The gluteus minimus and medius tendons are normal. No abnormal snapping with dynamic evaluation.
eBox 6-2 Sample Diagnostic Hip Ultrasound Report
Abnormal
Examination: Ultrasound of the Right Hip
History: Hip pain, evaluate for tendon tear
Findings: There is a partial tear of the adductor longus origin at the pubis. No evidence of full-thickness tear or tendon retraction. The common aponeurosis and rectus abdominis tendon are normal, as is the pubic symphysis.
The hip joint is normal without effusion or synovial hypertrophy. There is a possible tear of the anterior labrum. No paralabral cyst. No evidence of iliopsoas bursal distention or snapping iliopsoas tendon with dynamic imaging.
Evaluation of the lateral hip is normal. No evidence of abnormal bursal distention around the greater trochanter. The gluteus minimus and medius tendons are normal. No abnormal snapping with dynamic evaluation.
Hip Evaluation: Anterior
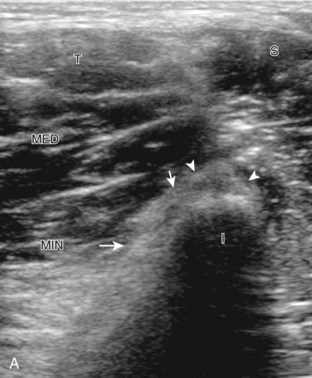
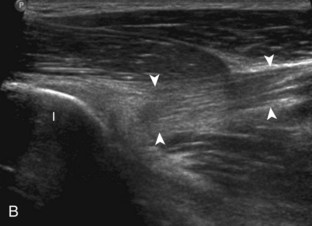
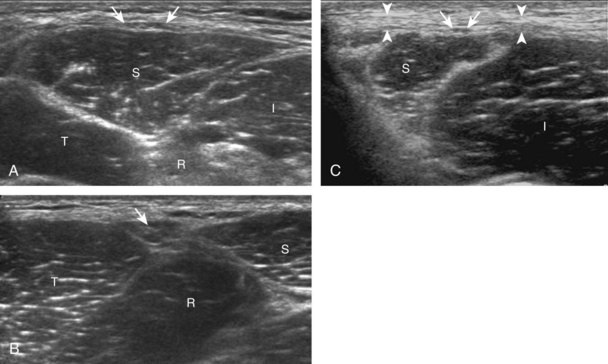
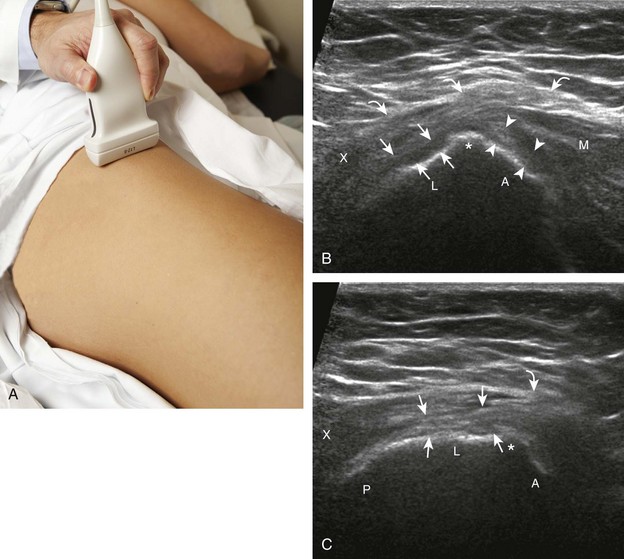
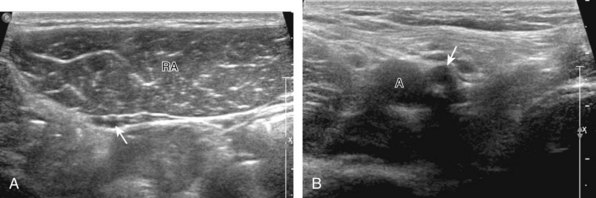
The primary structures evaluated include the hip joint and recess, iliopsoas tendon and bursa, proximal thigh musculature origin in the hip region (rectus femoris and sartorius), and pubic symphysis region. Depending on patient history and symptoms, all of these structures should be considered in the evaluation because symptoms may be referred and etiology multifactorial. Evaluation begins with the anterior hip with the transducer long axis to the femoral neck, which is in the oblique-sagittal plane (Fig. 6-2A). To find the femoral neck, one may initially image transversely over the femoral shaft to locate the curved and echogenic surface of the femur and then move the transducer proximally; once the bony protuberances of the greater and lesser trochanter are identified, the transducer is turned to the sagittal-oblique plane parallel to the femoral neck. The hip joint may also be located lateral to the femoral vasculature. The hip joint is identified long axis to the femoral neck by the characteristic bone contours of the femoral head, acetabulum, and femoral neck (see Fig. 6-2B to D). It is at this location superficial to the femoral neck where the anterior joint recess is evaluated for fluid or synovial abnormalities.1
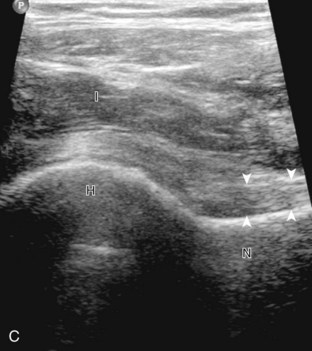
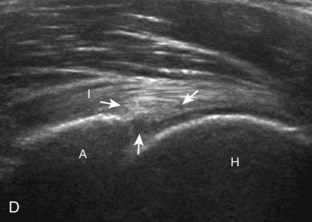
The anterior recess of the hip joint over the femoral neck is normally about 4 to 6 mm thick, and this can be explained anatomically.1 The anterior joint capsule extends inferiorly from the labrum and inserts at the intertrochanteric line; however, some fibers are reflected superiorly along the femoral neck to attach at the femoral head-neck junction (Fig. 6-3). Both the anterior and posterior layers measure 2 to 3 mm each in thickness; physiologic fluid between these layers should measure less than 2 mm, and typically no fluid is identified in the normal situation.1 The anterior capsule layer may be slightly thicker than the posterior layer as a result of capsular thickening from ligaments and the zona orbicularis, which encircles the capsule at the femoral head-neck junction. The posterior layer may demonstrate focal thickening at its attachment at the femoral head-neck junction. The normal anterior joint recess is usually concave or flat anteriorly, rather than convex. The true hyperechoic and fibrillar appearance of the joint capsule and its reflection is best appreciated when the femoral neck is perpendicular to the sound beam (see Fig. 6-2C); if imaged obliquely, the joint capsule may artifactually appear hypoechoic and may simulate fluid in echogenicity, especially in a patient with a large body habitus (see Fig. 6-2B). The femoral head and neck should be smooth, and the visualized portion of the hypoechoic hyaline cartilage that covers the femoral head should be uniform. The fibrocartilage labrum is hyperechoic and triangular and extends from the margins of the acetabulum (see Fig. 6-2D). The femoral head and neck are also evaluated in short axis to the femoral neck (Fig. 6-4).
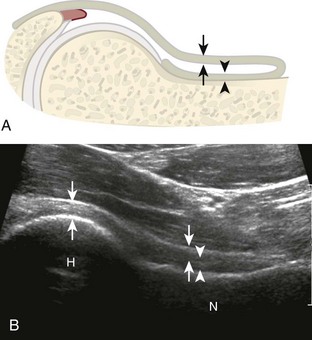
FIGURE 6-3 Anterior hip joint recess.
(Modified from an illustration by Carolyn Nowak, Ann Arbor, Mich. http://www.carolyncnowak.com/MedTech.html.)



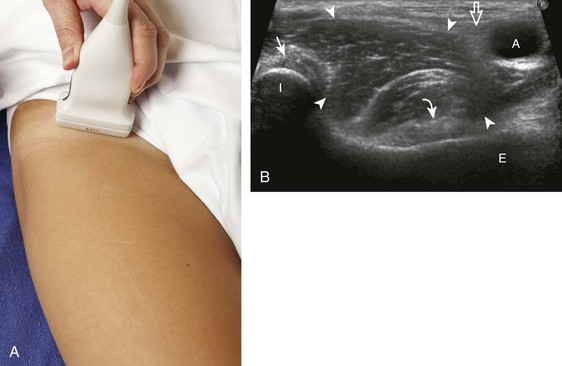
To evaluate the iliopsoas region, the transducer is first placed in the transverse plane over the femoral head because this bone landmark is easy to identify (see Fig. 6-4B). The transducer is then moved superiorly and angled parallel to the inguinal ligament (Fig. 6-5). The characteristic bone contours are seen along with the iliopsoas muscle and tendon, the rectus femoris origin at the anterior inferior iliac spine, and the external iliac vessels. As with imaging any tendon in short axis, toggling the transducer is often helpful to visualize the tendon as hyperechoic, especially because the iliopsoas normally courses deep toward the lesser trochanter and is oblique to the sound beam. The iliopsoas should be evaluated dynamically for tendon snapping (see Snapping Hip Syndrome later in the chapter). The anterior hip is also evaluated for iliopsoas bursa, which originates at the level of the femoral head and typically extends medial and possibly deep to the iliopsoas tendon. The transducer is also rotated 90 degrees to evaluate the iliopsoas tendon in long axis (see Fig. 6-2).
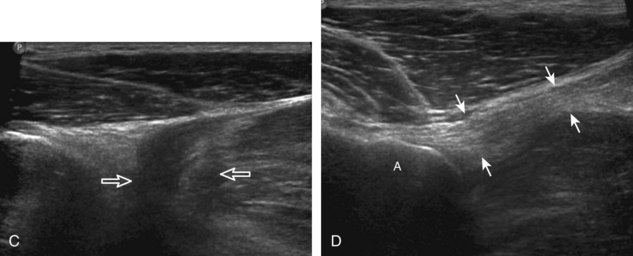
To further evaluate the rectus femoris origin, the transducer is positioned over the anterior inferior iliac spine in the transverse plane. The direct head is seen directly superficial to the anterior inferior iliac spine, whereas the indirect head is at the lateral aspect of the acetabulum (Fig. 6-6). When evaluating the direct head in long axis (see Fig. 6-6B), moving the transducer slightly laterally will show the indirect head coursing proximal and deep, appearing hypoechoic from anisotropy, and producing a characteristic refraction shadow (see Fig. 6-6C) (Video 6-1) . The transducer can be rotated in plane with the indirect head and moved over the lateral hip to identify the origin of the indirect head without artifact (see Fig. 6-6D) (Video 6-2)
. The transducer can be rotated in plane with the indirect head and moved over the lateral hip to identify the origin of the indirect head without artifact (see Fig. 6-6D) (Video 6-2) . The transducer is then returned to short axis relative to the rectus femoris direct head and moved proximally and laterally to visualize the sartorius and its origin on the anterior superior iliac spine (Fig. 6-7).
. The transducer is then returned to short axis relative to the rectus femoris direct head and moved proximally and laterally to visualize the sartorius and its origin on the anterior superior iliac spine (Fig. 6-7).
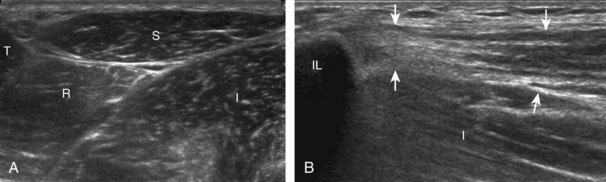
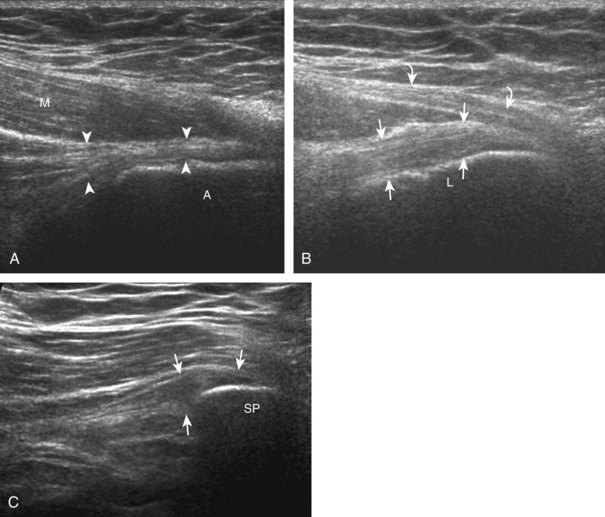
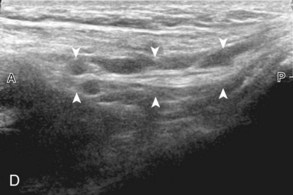
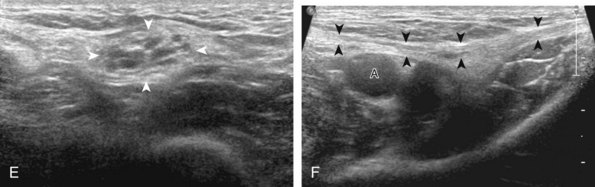
Evaluation for the lateral femoral cutaneous nerve begins with the transducer in the transverse plane over the proximal sartorius near the anterior superior iliac spine.10 As the transducer is moved distally, the lateral femoral cutaneous nerve can be seen as several nerve fascicles coursing over the sartorius from medial to lateral (Fig. 6-8A). More distally, the lateral femoral cutaneous nerve is identified in a triangular hypoechoic fatty space at the lateral aspect of the sartorius (see Fig. 6-8B) (Video 6-3 ).11 The transducer is then moved proximally to evaluate for potential nerve entrapment at the inguinal ligament (see Fig. 6-8C and D).12 The lateral femoral cutaneous nerve may branch proximal to the inguinal ligament and has a variable course; it may cross over the iliac crest, through the sartorius tendon, through the inguinal ligament, or under the inguinal ligament.9
).11 The transducer is then moved proximally to evaluate for potential nerve entrapment at the inguinal ligament (see Fig. 6-8C and D).12 The lateral femoral cutaneous nerve may branch proximal to the inguinal ligament and has a variable course; it may cross over the iliac crest, through the sartorius tendon, through the inguinal ligament, or under the inguinal ligament.9
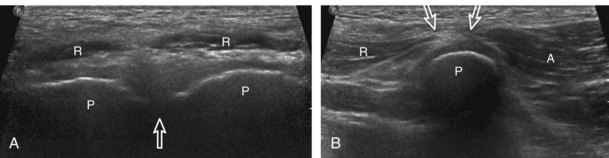
Although thigh evaluation is considered separately, patients with hip pain (especially sports-related pain) may have abnormalities at the adductor tendon origin and the rectus abdominis insertion, with possible abnormalities directly associated with the pubic symphysis.13 The transducer is placed in midline over the pubic symphysis, identified by its characteristic bone contours (Fig. 6-9A). The transducer is turned 90 degrees to evaluate the rectus abdominis in long axis and then rotated toward the adductors to evaluate the common aponeurosis and adductor tendon origin (see Fig. 6-9B).
Hip Evaluation: Lateral
To evaluate the soft tissues over the greater trochanter, bone landmarks are essential (Fig. 6-10). The patient rolls toward the opposite hip to access the posterolateral region of the hip and the transducer is placed over the lateral hip (Fig. 6-11A). To locate the greater trochanter, one begins in short axis to the femur as described earlier. With movement of the transducer cephalad, the bony protuberance of the greater trochanter is identified laterally. The key landmark is the apex of the greater trochanter between the anterior and lateral facets (see Fig. 6-11B).2 Posterior to the lateral facet is the rounded posterior facet of the greater trochanter. The gluteus minimus tendon is identified over the anterior facet, the distal gluteus medius over the lateral facet, and the gluteus maximus over the posterior facet. To confirm that the apex between the lateral and anterior facets is correctly identified, the soft tissues superficial to the gluteus medius and minimus should be evaluated. Superficial to the gluteus medius tendon over the lateral facet one should identify the iliotibial tract, a hyperechoic band of tissue, which is a continuation of the fascial layers that envelop the gluteus maximus posteriorly and the tensor fascia latae anteriorly (see Fig. 6-10). Superficial to the gluteus minimus tendon over the anterior facet is seen the hypoechoic muscle of the gluteus medius and iliotibial tract. Each greater trochanter facet should be evaluated separately in short (see Fig. 6-11) and long axis (Fig. 6-12); the transducer should be positioned so that the cortex of each individual facet is perpendicular to the sound beam to eliminate anisotropy of each overlying tendon (see Fig. 6-11B and C). Evaluation includes assessment for the subgluteus minimus bursa, subgluteus medius bursa, and trochanteric (subgluteus maximus) bursa, which are located between each tendon and their respective greater trochanter facet.2 Because the trochanteric bursa is located between the gluteus maximus and posterior facet, it is essential to position the transducer posteriorly so as not to overlook bursal distention. When distended, the trochanteric bursa may extend laterally between the gluteus medius tendon and overlying iliotibial tract. For evaluation of the gluteus minimus tendon in long axis, the transducer is first positioned over the anterior facet in short axis as described previously and turned 90 degrees (see Fig. 6-12A). The same technique is used over the lateral facet to evaluate the gluteus medius tendon in long axis (see Fig. 6-12B). Because the gluteus medius tendon is attached to two facets (lateral and superoposterior), the transducer should be moved cephalad and posterior to visualize the full extent of the gluteus medius tendon attachment (see Fig. 6-12C).
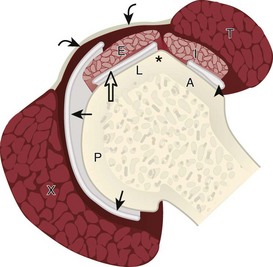
FIGURE 6-10 Greater trochanter anatomy.
(Modified from an illustration by Carolyn Nowak, Ann Arbor, Mich. http://www.carolyncnowak.com/MedTech.html.)
Hip Evaluation: Posterior
Evaluation of the posterior hip and pelvis is not typically considered part of a routine hip evaluation but rather is guided by patient history and symptoms. Structures of interest include the sacroiliac joints, piriformis, superior gemellus, obturator internus, inferior gemellus, and quadriceps femoris. Evaluation can begin with the sacroiliac joint by first positioning the transducer in midline over the sacrum (Fig. 6-13) and then moving the transducer laterally to visualize the posterior sacral foramina and more laterally to view the sacroiliac joint (Video 6-4) .14 The posterior sacral foramina are differentiated from the sacroiliac joint by their more medial location as well as the characteristic focal disruptions in the cortex when scanning superior to inferior, which is in contrast to the more lateral and linear disruption of the sacroiliac joint. The superior aspect of the sacroiliac joint is widened at the fibrocartilage or ligamentous articulation (see Fig. 6-13A), whereas the more inferior true synovial articulation is narrow (see Fig. 6-13B).
.14 The posterior sacral foramina are differentiated from the sacroiliac joint by their more medial location as well as the characteristic focal disruptions in the cortex when scanning superior to inferior, which is in contrast to the more lateral and linear disruption of the sacroiliac joint. The superior aspect of the sacroiliac joint is widened at the fibrocartilage or ligamentous articulation (see Fig. 6-13A), whereas the more inferior true synovial articulation is narrow (see Fig. 6-13B).
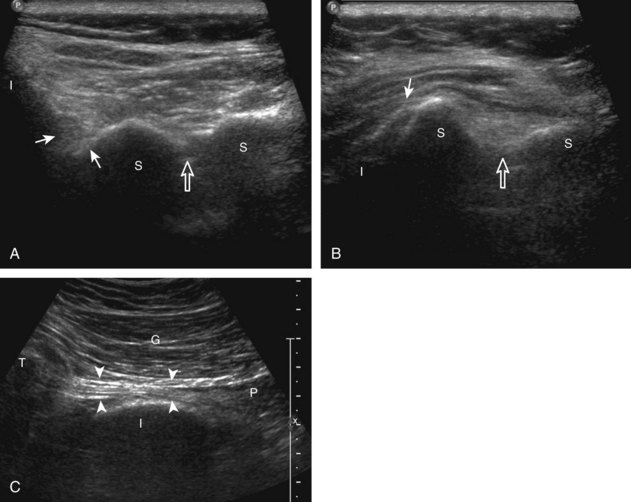
To identify the piriformis, a curvilinear transducer with a frequency of less than 10 MHz is essential given the required depth of penetration. The transducer is first positioned in the transverse plane over the sacroiliac joint, as described previously, and then moved inferior into the greater sciatic foramen and angled inferiorly and laterally toward the greater trochanter to identify the piriformis in long axis (see Fig. 6-13C).15,16 The muscle belly will be located medial to the ilium, while the tendon will be seen directly over the ilium extending to the greater trochanter. Passive hip rotation will assist in its identification because of its movement (Videos 6-5 and 6-6) .
.
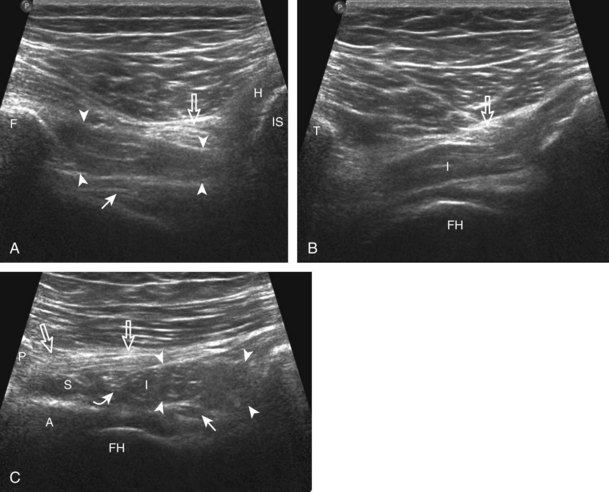
To identify the quadratus femoris, obturators, and gemelli, examination can begin in the transverse plane at the level of the hamstring origin (Fig. 6-14A). Deep to the sciatic nerve between the ischium and proximal femur is located the quadratus femoris and obturator externus. More cephalad (see Fig. 6-14B), the inferior gemellus muscle is seen, which has a slightly different course compared with the quadratus femoris as it extends deep to its lateral insertion on the medial aspect of the greater trochanter. In their short axis, from cephalad to caudal, the superior gemellus, obturator internus, inferior gemellus, and quadratus femoris are identified deep to the sciatic nerve (see Fig. 6-14C).
Inguinal Region Evaluation
Sonographic evaluation of the inguinal region for hernias may incorporate evaluation of the anterior abdominal wall for abnormalities.8 Evaluation is begun in the transverse plane over the mid-abdomen below the umbilicus with the patient supine. At this location, the linea alba is seen as a hyperechoic fascial layer between the rectus abdominis muscles. The transducer is then moved to the lateral margin of a rectus abdominis muscle. As the transducer is moved inferior in the transverse plane, the inferior epigastric artery can be identified beneath the rectus abdominis (Fig. 6-15A, online). It is here at the lateral margin of the rectus abdominis that spigelian hernias are seen, between the rectus abdominis muscle and lateral abdominal musculature. More inferiorly, the site where the inferior epigastric artery joins the external iliac artery is a very important landmark; just lateral and superior to this location is the deep inguinal ring (see Fig. 6-15B, online). Hernias that originate lateral to the inferior epigastric artery at the deep inguinal ring and extend superficially and medially within the inguinal canal are indirect inguinal hernias. Hernias that originate medial to the inferior epigastric origin in the Hesselbach triangle and move in an anterior direction are direct hernias.8 At the deep inguinal ring, the transducer is then angled toward the pubis, parallel and just superior to the inguinal ligament, and long axis to the inguinal canal (see Fig. 6-15C, online). In male patients, the serpiginous and mixed-echogenicity spermatic cord can be identified (see Fig. 6-15D and E, online). In this location, the patient is asked to tighten the stomach or perform the Valsalva maneuver (forced expiration against a closed airway) to evaluate for transient herniation of intra-abdominal structures or tissue; the patient can be asked to blow against the back of the hand and puff the cheeks outward. This maneuver is also repeated with the transducer more medial, at the pubis, to evaluate for direct hernias. It is also important to image the Hesselbach triangle at its medial and superior aspects both in long and short axis to the inguinal canal for complete evaluation because the cephalocaudal extent of this triangle is greatest medially. Evaluation for inguinal hernias should also be completed in the sagittal plane. For example, when imaging the inguinal canal and spermatic cord (in males) in short axis, an indirect inguinal hernia will be seen moving in and out of the ultrasound plane displacing the spermatic cord. Similar to the transverse plane, a direct hernia will appear as focal abnormal anterior movement. After returning the transducer long axis to the inguinal ligament, the transducer is moved distally over the common femoral artery just beyond the inguinal ligament to evaluate for femoral hernias. Although the causes of “sports hernia” are debated, evaluation for hip or groin pain in the athlete should include the pubis symphyseal region, the hip joint, and the labrum (see earlier), in addition to evaluation for inguinal region hernias.17

Thigh Evaluation: Anterior
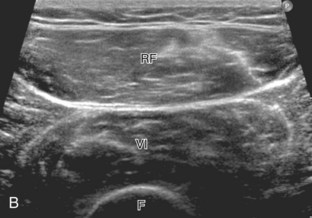
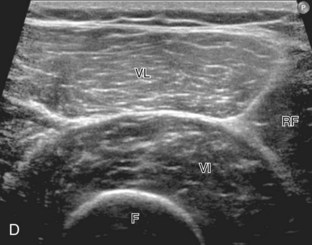
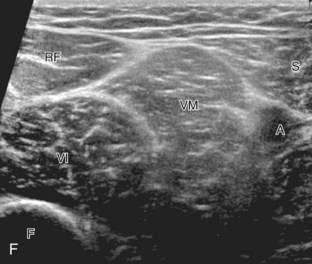
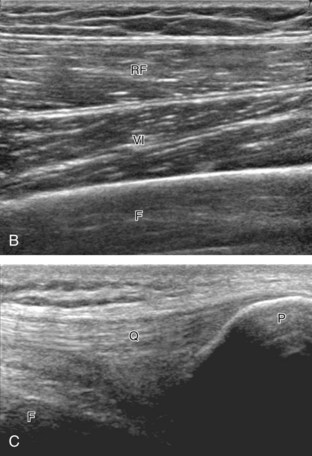
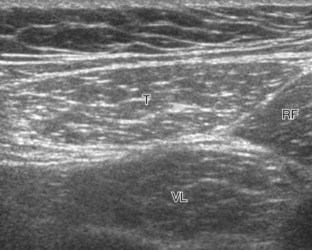
Structures of interest anteriorly in the thigh include the four muscles that make up the quadriceps femoris. Examination is begun in the transverse plane over the mid-anterior thigh, where the four individual muscles can be identified (Fig. 6-16A) (Videos 6-7 and 6-8) . Directly below the transducer and most superficial is the rectus femoris muscle (see Fig. 6-16B). Deep to this and immediately adjacent to the femur is the vastus intermedius. Lateral to these two structures is the vastus lateralis (see Fig. 6-16C and D), and medial is the vastus medialis (see Fig. 6-16E and F). Muscle at ultrasound is predominantly hypoechoic, although interspersed hyperechoic septa are identified. The quadriceps femoris is then evaluated in long axis (Fig. 6-17). As one moves the transducer distally, the rectus femoris tapers to a tendon, followed by the vastus musculature, which forms the trilaminar quadriceps tendon that inserts on the superior pole of the patella. The superficial layer of the distal quadriceps tendon is made up of the rectus femoris, the middle layer is composed of both the vastus medialis and lateralis tendons, and the deep layer is made up of the vastus intermedius tendon. Some quadriceps tendon fibers continue over the patella (termed the prepatellar quadriceps continuation) to attach to the tibial tuberosity by means of the patellar tendon.18 The distal tapering appearance of the rectus femoris is best appreciated in long axis in the sagittal plane. The individual muscles of the quadriceps can then be evaluated more proximally. As described earlier, the rectus femoris tendon proximally originates at the ilium (see Fig. 6-6), where its direct head originates from the anterior inferior iliac spine and the indirect or reflected head originates at the lateral aspect. In the thigh, the direct head flattens superficially, the indirect head continues within the central region of the rectus femoris, and more distally a posterior aponeurosis forms.4 The adjacent tensor fasciae latae is seen lateral to the rectus femoris muscle (Fig. 6-18); the fascia of the tensor fascia latae continues laterally as the iliotibial tract (see Fig. 6-10).
. Directly below the transducer and most superficial is the rectus femoris muscle (see Fig. 6-16B). Deep to this and immediately adjacent to the femur is the vastus intermedius. Lateral to these two structures is the vastus lateralis (see Fig. 6-16C and D), and medial is the vastus medialis (see Fig. 6-16E and F). Muscle at ultrasound is predominantly hypoechoic, although interspersed hyperechoic septa are identified. The quadriceps femoris is then evaluated in long axis (Fig. 6-17). As one moves the transducer distally, the rectus femoris tapers to a tendon, followed by the vastus musculature, which forms the trilaminar quadriceps tendon that inserts on the superior pole of the patella. The superficial layer of the distal quadriceps tendon is made up of the rectus femoris, the middle layer is composed of both the vastus medialis and lateralis tendons, and the deep layer is made up of the vastus intermedius tendon. Some quadriceps tendon fibers continue over the patella (termed the prepatellar quadriceps continuation) to attach to the tibial tuberosity by means of the patellar tendon.18 The distal tapering appearance of the rectus femoris is best appreciated in long axis in the sagittal plane. The individual muscles of the quadriceps can then be evaluated more proximally. As described earlier, the rectus femoris tendon proximally originates at the ilium (see Fig. 6-6), where its direct head originates from the anterior inferior iliac spine and the indirect or reflected head originates at the lateral aspect. In the thigh, the direct head flattens superficially, the indirect head continues within the central region of the rectus femoris, and more distally a posterior aponeurosis forms.4 The adjacent tensor fasciae latae is seen lateral to the rectus femoris muscle (Fig. 6-18); the fascia of the tensor fascia latae continues laterally as the iliotibial tract (see Fig. 6-10).




Thigh Evaluation: Medial
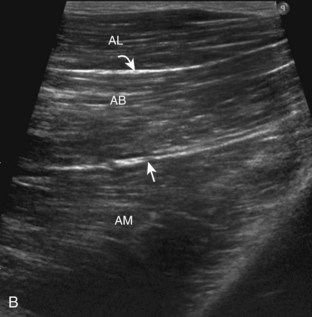
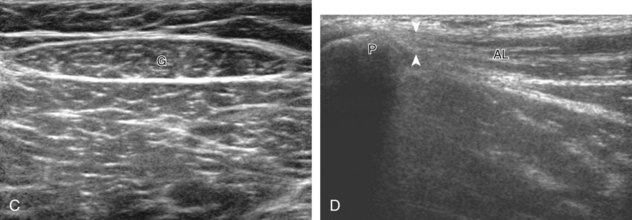
Structures of interest in the medial thigh include the femoral nerve, artery, and vein and the sartorius, gracilis, and adductor musculature. Ultrasound examination is begun similar to the anterior thigh for orientation, with initial identification of the rectus femoris muscle. The transducer is then moved cephalad into the medial upper thigh (see Fig. 6-16E). The femoral artery is identified at the medial aspect of the rectus femoris and vastus medialis muscles and is a very helpful landmark (Fig. 6-19A). Directly superficial to the femoral artery is the sartorius muscle. Medial and posterior to these structures are the adductor muscles (see Fig. 6-19B). The most anterior is the adductor longus muscle, next posterior is the adductor brevis muscle, and most posterior and largest is the adductor magnus muscle. Between these respective muscles are located the anterior and posterior branches of the obturator nerve. Superficial and medial to the adductor muscles is the gracilis muscle, just below the subcutaneous tissues (see Fig. 6-19C). For each of these medial thigh muscles, the proximal to distal extents can be visualized in short axis. The transducer can also be turned in long axis over each muscle to visualize the proximal origins and distal attachments (see Fig. 6-19D).