Chapter 3 Gastrointestinal tract
Methods of imaging the gastrointestinal tract
Ambrosini R., Barchiesi A., Di Mizio V., et al. Inflammatory chronic disease of the colon: how to image. Eur. J. Radiol.. 2007;61(3):442-448.
Brochwicz-Lewinski M.J., Paterson-Brown S., Murchison J.T. Small bowel obstruction the water soluble follow-through revisited. Clin. Radiol.. 2003;58(5):393-397.
Gasparaitis A.E., MacEneaney P. Enteroclysis and computed tomography enteroclysis. Gastroenterol. Clin. North Am.. 2002;31(3):715-730.
Introduction to Contrast Media
BARIUM
Barium suspension is made up from pure barium sulphate. (Barium carbonate is poisonous.) The particles of barium must be small (0.1–3 µm), since this makes them more stable in suspension. A non-ionic suspension medium is used, for otherwise the barium particles would aggregate into clumps. The resulting solution has a pH of 5.3, which makes it stable in gastric acid.
There are many varieties of barium suspensions in use. Exact formulations are secret. In most situations the preparation will be diluted with water to give a lower density (Table 3.1).
Table 3.1 Barium suspensions and dilutions with water to give a lower density
| Proprietary name | Density (w/v) – use |
|---|---|
| Baritop 100 | 100% – all parts gastrointestinal tract |
| EPI-C | 150% – large bowel |
| E-Z-Cat | 1–2% – computed tomography of gastrointestinal tract |
| E-Z HD | 250% – oesophagus, stomach and duodenum |
| E-Z Paque | 100% – small intestine |
| Micropaque DC | 100% – oesophagus, stomach and duodenum |
| Micropaque liquid | 100% – small and large bowel |
| Micropaque powder | 76% – small and large bowel |
| Polibar | 115% – large bowel |
| Polibar rapid | 100% – large bowel |
Advantages
Disadvantages
Complications
For further complications (e.g. constipation and impaction), see the specific procedure involved.
Water-Soluble Contrast Agents
GASES
Pharmacological Agents
Hyoscine-N-butyl bromide (Buscopan)
Glucagon
This polypeptide hormone produced by the alpha cells of the islets of Langerhans in the pancreas has a predominantly hyperglycaemic effect but also causes smooth muscle relaxation.
General points
CONTRAST SWALLOW
Contrast medium
Equipment
Rapid serial radiography (6 frames per s) or video recording may be required for assessment of the laryngopharynx and upper oesophagus during deglutition.
Patient preparation
None (but as for barium meal if the stomach is also to be examined – see p. 57).
Preliminary film
A control film is advised prior to a water-soluble study if perforation is suspected.
Technique
Modification of technique
Recently, it has been proposed that pull-back studies are not necessary in the majority of children, as tracheo-oesophageal fistulas can usually be demonstrated on standard contrast swallow examination, providing the oesophagus is distended well with contrast media.1 Pull-back studies are still necessary for intubated patients, or those who are at high risk of aspiration. It is important to remember that fistulas are usually quite high, and the orifice can be occluded by an endotracheal tube. This can prevent the fistula being opacified. This can be rectified by altering the patients position, or slightly withdrawing the ET tube.
Barium Meal
Technique
The double contrast method (Fig. 3.1):
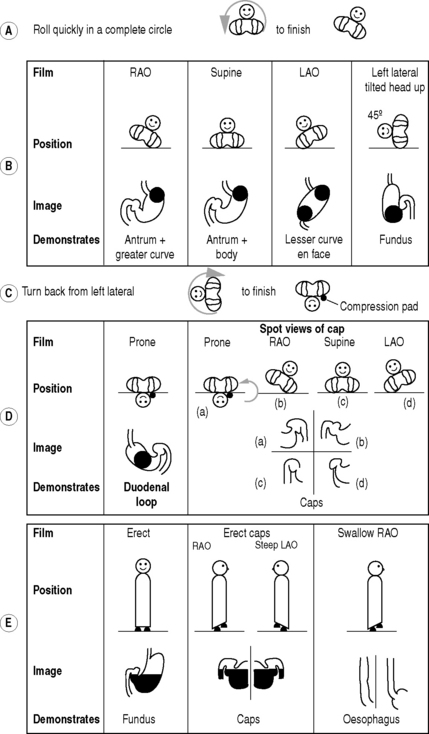
 = Barium
= BariumFilms
From the left lateral position the patient returns to a supine position and then rolls onto the left side and over into a prone position. This sequence of movements is required to avoid barium flooding into the duodenal loop, which would occur if the patient were to roll onto the right side to achieve a prone position.
Modification of technique for young children
In newborn infants with upper intestinal obstruction, e.g. duodenal atresia, the diagnosis may be confirmed if 20 ml of air is injected down the nasogastric tube (which will almost certainly have already been introduced by the medical staff). If the diagnosis remains in doubt, it can be replaced by a positive contrast agent (dilute barium or LOCM if the risk of aspiration is high).
Aftercare
BARIUM FOLLOW-THROUGH
Contraindications
Contrast medium
In situations where barium is contraindicated, non-ionic water-soluble solutions have been shown to be a satisfactory alternative.1
Films
Ha H.K., Shin J.H., Rha S.E., et al. Modified small bowel follow through: use of methylcellulose to improve bowel transradiance and prepare barium suspension. Radiology. 1999;211:197-201.
Summers D.S., Roger M.D., Allan P.L., et al. Accelerating the transit time of barium sulphate suspensions in small bowel examinations. Eur. J. Radiol.. 2007;62(1):122-125.
Small-Bowel Enema
Indications and Contraindications
These are the same as for a barium follow-through. In some departments it is only performed in the case of an equivocal follow-through.
Equipment
Patient preparation
Immediately before the examination the pharynx is anaesthetized with lidocaine spray.



