CHAPTER 49 Forearm
SKIN AND SOFT TISSUE
SKIN
Cutaneous vascular supply
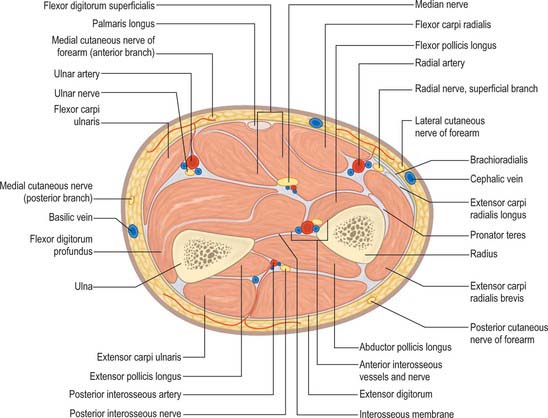
Fasciocutaneous perforators from the radial artery supply the lateral two-thirds of the anterior surface of the forearm, the lateral (radial) border and the posterior one-quarter of the forearm (except in the distal third) (see Fig. 45.4). These perforators pass in the intermuscular fascia between brachioradialis and flexor carpi radialis and between flexor carpi radialis and flexor digitorum superficialis (see Fig. 49.17). Within the territory of the radial artery is the area of the largest fasciocutaneous perforator, which has recently been named the inferior cubital artery. It extends from the distal apex of the antecubital fossa to midway down the forearm. Fasciocutaneous perforators from the ulnar artery supply an anatomical area which extends from the cubital fossa to the wrist, and from the medial (ulnar) third of the anterior aspect of the forearm around the medial border to the medial one-quarter of the posterior surface of the forearm (see Fig. 49.17, Fig. 45.4).
The distal third of the lateral (radial) aspect of the forearm is supplied by the terminal perforating branches of the anterior interosseous artery (see Fig. 45.4).
The central half of the posterior surface of the forearm, from the lateral edge of extensor digitorum, just below the lateral epicondyle of the humerus, to the wrist, is supplied by fasciocutaneous perforators which arise from the posterior interosseous artery. They reach the skin by passing along the intermuscular fascia between extensor carpi ulnaris and extensor digit minimi (see Fig. 49.17, Fig. 45.4).
For a detailed account of the cutaneous blood supply to the forearm, see Cormack & Lamberty (1994) and the translated works of Salmon (1994).
Cutaneous innervation
The anterior aspect of the forearm is supplied by the anterior branches of the medial and lateral cutaneous nerves of the forearm (see Fig. 45.15). The medial and lateral regions of the posterior aspect of the forearm are supplied by the posterior branches of the medial and lateral cutaneous nerves of the forearm respectively. The central part of the posterior aspect of the forearm is supplied by the posterior cutaneous nerve of the forearm.
SOFT TISSUE
Interosseous membrane
Oblique cord
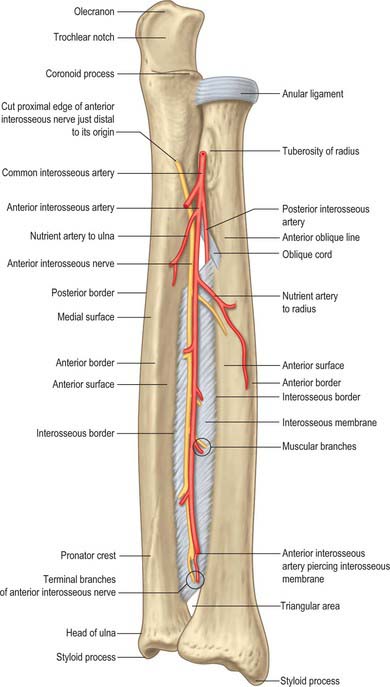
The oblique cord is a small inconstant flat fascial band on the deep head of supinator (Fig. 49.1). It extends from the lateral side of the ulnar tuberosity to the radius a little distal to its tuberosity. Its fibres are at right angles to those in the interosseous membrane. Its functional significance is dubious.
Interosseous membrane
The interosseous membrane is a broad, thin, collagenous sheet (Fig. 49.1). Its fibres slant distomedially between the radial and ulnar interosseous borders, and its distal part is attached to the posterior division of the radial border. Two or three posterior bands occasionally descend distolaterally across the other fibres. The membrane is deficient proximally, starting 2 or 3 cm distal to the radial tuberosity, and broader at midlevel. An oval aperture near its distal margin conducts the anterior interosseous vessels to the back of the forearm, and the posterior interosseous vessels pass through a gap between its proximal border and the oblique cord.
The membrane provides attachments for the deep forearm muscles and connects the radius and ulna. Its fibres appear to transmit forces which act proximally from the hand to the radius, thence to the ulna and humerus. However the hand is usually pronated when subject to these forces, and the membrane is relaxed in complete pronation and supination: the interosseous membrane is only tense when the hand is midway between prone and supine positions. Moreover, the radius can transmit substantial forces directly to the humerus. Anteriorly, in its proximal three-quarters, the membrane is related laterally to flexor pollicis longus and medially to flexor digitorum profundus, and between them to the anterior interosseous vessels and nerve. In its distal quarter it is related to pronator quadratus. Its posterior relations are supinator, abductor pollicis longus, extensors pollicis brevis, longus and indicis and, near the carpus, the anterior interosseous artery and posterior interosseous nerve.
Compartments of the forearm
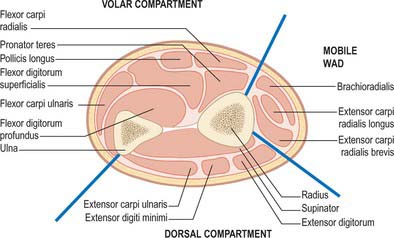
The antebrachial fascia (deep fascia of the forearm), which is continuous above with the brachial fascia, is a dense general sheath for muscles, collectively and individually, in this region. It is attached to the olecranon and posterior border of the ulna. From its deep surface septa pass between muscles, providing partial attachment for them, and some of these septa reach bone. Muscles also arise from its internal aspect, especially in the upper forearm. This deep fascia, together with the interosseous membrane and fibrous intermuscular septa, divide the forearm into a number of compartments. These are the superficial and deep flexor (anterior) compartments, the extensor (posterior compartment) and a proximolateral compartment known as the mobile wad (encompassing brachioradialis and extensors carpi radialis longus and brevis) (Fig. 49.2). The fascia is much thicker posteriorly and in the lower forearm. It is strengthened above by tendinous fibres from biceps and triceps. Near the wrist, two localized thickenings, the flexor and extensor retinacula, retain the digital tendons in position (p. 879). Vessels and nerves pass through apertures in the fascia. One large aperture anterior to the elbow transmits a venous communication between superficial and deep veins.
BONE
RADIUS
The radius is the lateral bone of the forearm (Fig. 49.3, Fig. 49.4, Fig. 49.5). It has expanded proximal and distal ends; the distal is much the broader. The shaft widens rapidly towards its distal end, is convex laterally and concave anteriorly in its distal part.
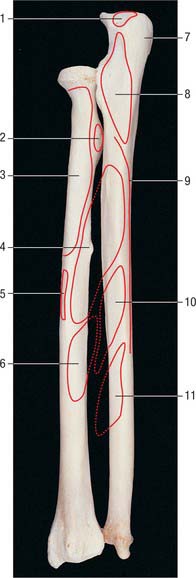

Fig. 49.5 Proximal end of left radius: anterior view. 1. Head. 2. Radial tuberosity. 3. Shaft. 4. Neck.
Shaft
The shaft has a lateral convexity, and is triangular in section (Fig. 49.1). The interosseous border is sharp, except for two areas: proximally, near the tuberosity; and distally, where the interosseous border is the posterior margin of a small, elongated, triangular area, proximal to the ulnar notch. These two areas form the so-called medial surface. The interosseous membrane is attached to its distal three-fourths, and connects the radius to the ulna. The anterior border is obvious at both ends, but rounded and indefinite between them. It descends laterally from the anterolateral part of the tuberosity as the anterior oblique line, which distally becomes a sharp, palpable crest along the lateral margin of the anterior surface. The posterior border is well defined only in its middle third: proximally it ascends medially towards the posteroinferior part of the tuberosity, and distally it is merely a rounded ridge. The anterior surface, between anterior and interosseous borders, is concave transversely and shows a distal forward curvature. Near its midpoint there is a proximally directed nutrient foramen and canal. The posterior surface, between interosseous and posterior borders, is largely flat but may be slightly hollow in the proximal area. The lateral surface is gently convex. Proximally, due to the obliquity of the anterior and posterior borders, it encroaches on the anterior and posterior aspects and is here slightly rough. A finely irregular oval area occurs near the midshaft, and beyond it the surface is smooth.
Distal end
The distal end of the radius (Fig. 49.6) is the widest part. It is four-sided in section. The lateral surface is slightly rough, projecting distally as a styloid process which is palpable when tendons around it are slack. The smooth carpal articular surface is divided by a ridge into medial and lateral areas. The medial is quadrangular, whereas the lateral is triangular and curves on to the styloid process. The anterior surface is a thick, prominent ridge, palpable even through overlying tendons, 2 cm proximal to the thenar eminence. The medial surface is the ulnar notch, which is smooth and anteroposteriorly concave for articulation with the head of the ulna. The posterior surface displays a palpable dorsal tubercle (Lister’s tubercle), which is limited medially by an oblique groove and is in line with the cleft between the index and middle fingers. Lateral to the tubercle there is a wide, shallow groove, divided by a faint vertical ridge.
Muscle, ligament and articular attachments
The proximal two-thirds of the anterior surface provides an extensive area for attachment of flexor pollicis longus, which conceals the nutrient foramen. Pronator quadratus is attached to the distal quarter, and pronator teres is attached to a rough area near the midpoint of its lateral surface, at its maximal curvature. Proximally, the lateral surface widens into a long V-shaped area for supinator (Fig. 49.3, Fig. 49.4). Distal to pronator teres, the lateral surface is covered by tendons of the radial extensors. On the posterior surface, abductor pollicis longus is attached proximally and, more distally, extensor pollicis brevis. The remaining surface is devoid of attachments and covered by the long and short extensors of the thumb.
The radial styloid process projects beyond that of the ulna, its apex concealed by the tendons of abductor pollicis longus and extensor pollicis brevis. The lateral radiocarpal ligament is attached to its tip. The lateral surface, near the styloid process, receives the attachment of brachioradialis and is crossed obliquely, downwards and forwards, by the tendons of abductor pollicis longus and extensor pollicis brevis. The terminal ridge on the anterior surface of the lower end is an attachment for the palmar radiocarpal ligament. The base of the triangular articular disc of the inferior radio-ulnar joint is attached to a smooth ridge distal to the ulnar notch. From the latter, a narrow protrusion of synovial membrane extends proximally anterior to the lower end of the interosseous membrane (p. 839). The lateral part of the carpal articular surface articulates with the scaphoid, and the medial part with the lateral part of the lunate. In full adduction, the proximal surface of the lunate is wholly in contact with the radius.
Vascular supply
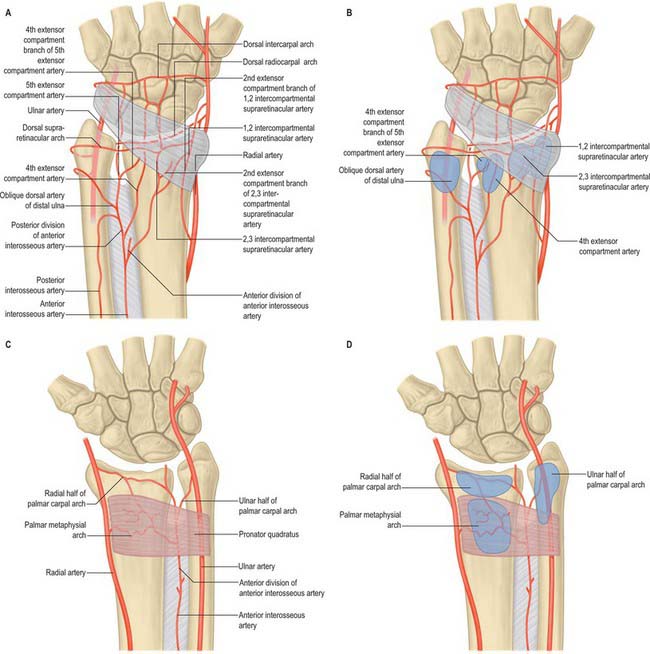
The dorsal metaphysial supply of the distal radius is of particular importance to reconstructive hand surgeons because of its potential use in raising vascularized pedicled bone grafts (Fig. 49.7). Consistent branches connecting the anterior interosseous artery proximally to the dorsal carpal arch distally pass through the fourth and fifth extensor compartments of the wrist and provide metaphysial nutrient arteries. Intercompartmental vessels send nutrient arteries to the radius through the retinaculum between the first and second dorsal compartments, and the second and third dorsal compartments. These vessels originate from the radial artery and anterior interosseous arteries respectively, and anastomose with the dorsal carpal arch. For an anatomical description detailing the practical application of such pedicled bone grafts see Sheetz et al (1995).
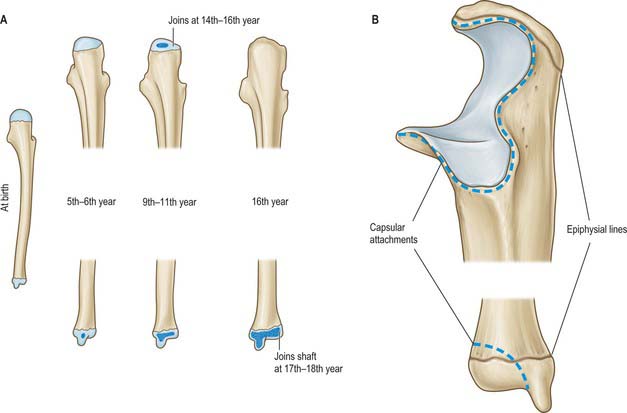
Ossification
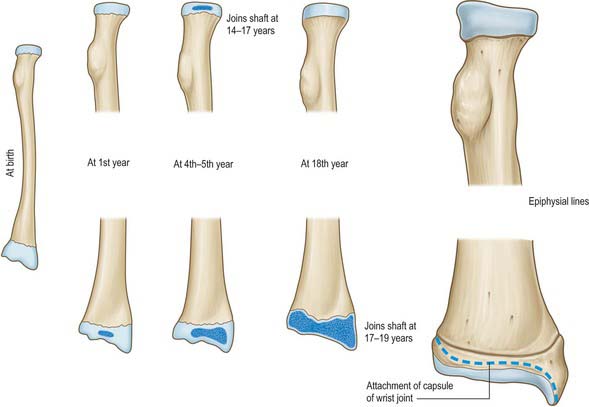
The radius ossifies from three centres. One appears centrally in the shaft in the eighth week of fetal life, and the others appear in each end (Fig. 49.8, Fig. 49.9). Ossification begins in the distal epiphysis towards the end of the first postnatal year, and in the proximal epiphysis during the fourth year in females, and fifth in males. The proximal epiphysis fuses in the 14th year in females, 17th in males, and the distal in the 17th and 19th years respectively. A fourth centre sometimes appears in the tuberosity at about the 14th or 15th year.

ULNA
The ulna is medial to the radius in the supinated forearm (Fig. 49.3, Fig. 49.4). Its proximal end is a massive hook which is concave forwards (Fig. 49.10). The lateral border of the shaft is a sharp interosseous crest. The bone diminishes progressively from its proximal mass throughout almost its whole length, but at its distal end expands into a small rounded head and styloid process. The shaft is triangular in section but has no appreciable double curve. In its whole length it is slightly convex posteriorly. Mediolaterally, its profile is sinuous. The proximal half has a slight laterally concave curvature, and the distal half a medially concave curvature.

Proximal end
The proximal end has large olecranon and coronoid processes and trochlear and radial notches which articulate with the humerus and radius (Fig. 49.10). The olecranon is more proximal and is bent forwards at its summit like a beak, which enters the humeral olecranon fossa in extension. Its posterior surface is smooth, triangular and subcutaneous, and its proximal border underlies the ‘point’ of the elbow. In extension it can be felt near a line joining the humeral epicondyles, but in flexion it descends, so that the three osseous points form an isosceles triangle. Its anterior, articular surface forms the proximal area of the trochlear notch. Its base is slightly constricted where it joins the shaft and is the narrowest part of the proximal ulna. The coronoid process projects anteriorly distal to the olecranon. Its proximal aspect forms the distal part of the trochlear notch. On the lateral surface, distal to the trochlear notch, there is a shallow, smooth, oval radial notch which articulates with the radial head. Distal to the radial notch the surface is hollow to accommodate the radial tuberosity during pronation and supination. The anterior surface of the coronoid is triangular. Its distal part is the tuberosity of the ulna. Its medial border is sharp and bears a small tubercle proximally.
The trochlear notch articulates with the trochlea of the humerus. It is constricted at the junction of the olecranon and coronoid processes, where their articular surfaces may be separated by a narrow rough non-articular strip. A smooth ridge, adapted to the groove on the humeral trochlea, divides the notch into medial and lateral parts. The medial fits into the trochlear flange. The radial notch, an oval or oblong proximal depression on the lateral aspect of the coronoid process, articulates with the periphery of the radial head, and is separated from the trochlear notch by a smooth ridge (Fig. 49.10).
Shaft
The shaft is triangular in section in its proximal three-fourths, but distally is almost cylindrical (Fig. 49.3, Fig. 49.4). It has anterior, posterior and medial surfaces and interosseous, posterior and anterior borders. The interosseous border is a conspicuous lateral crest in its middle two-fourths. Proximally it becomes the supinator crest, which is continuous with the posterior border of a depression distal to the radial notch. Distally, it disappears. The rounded anterior border starts medial to the ulnar tuberosity, descends backwards, and is usually traceable to the base of the styloid process. The posterior border, also rounded, descends from the apex of the posterior aspect of the olecranon, and curves laterally to reach the styloid process. It is palpable throughout its length in a longitudinal furrow which is most obvious when the elbow is fully flexed.
The anterior surface, between the interosseous and anterior borders, is longitudinally grooved, sometimes deeply (Fig. 49.3). Proximal to its midpoint there is a nutrient foramen, which is directed proximally and contains a branch of the anterior interosseous artery. Distally, it is crossed obliquely by a rough, variable prominence, descending from the interosseous to the anterior border. The medial surface, between the anterior and posterior borders, is transversely convex and smooth. The posterior surface, between the posterior and interosseous borders, is divided into three areas (Fig. 49.4). The most proximal is limited by a sometimes faint oblique line ascending laterally from the junction of the middle and upper thirds of the posterior border to the posterior end of the radial notch. The region distal to this line is divided into a larger medial and narrower lateral strip by a vertical ridge, usually distinct only in its proximal three-fourths.
Distal end
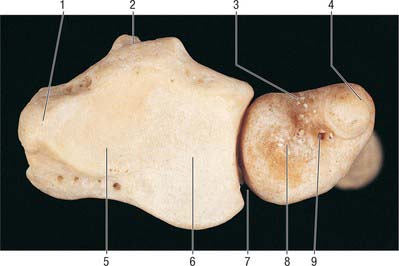
The distal end is slightly expanded and has a head and styloid process. The head is visible in pronation on the posteromedial carpal aspect, and can be gripped when the supinated hand is flexed. Its lateral convex articular surface fits the radial ulnar notch. Its smooth distal surface (Fig. 49.6) is separated from the carpus by an articular disc, the apex of which is attached to a rough area between the articular surface and styloid process. The latter, a short, round, posterolateral projection of the distal end of the ulna, is palpable (most readily in supination) about 1 cm proximal to the plane of the radial styloid. A posterior vertical groove is present between the head and styloid process.
Vascular supply
Multiple metaphysial nutrient foramina transmit branches of the radial, ulnar, anterior and posterior interosseous arteries (Fig. 49.7). These vessels give off a number of smaller segmental branches. Usually one, but occasionally two, major nutrient diaphysial foramina are located on the anterior surface of the bone, directed proximally toward the elbow. A network of small fascioperiosteal and musculoperiosteal branches given off from the compartmental vessels reaches the bone via septal and muscular attachments.
Ossification
The ulna ossifies from four main centres, one each in the shaft and distal end and two in the olecranon (Fig. 49.11). Ossification begins in the midshaft about the eighth fetal week, and extends rapidly. In the fifth (females) and sixth (males) years, a centre appears in the distal end, and extends into the styloid process. The distal olecranon is ossified as an extension from the shaft, the remainder from two centres, one for the proximal trochlear surface, and the other for a thin scale-like proximal epiphysis on its summit. The latter appears in the ninth year in females, 11th in males. The whole proximal epiphysis has joined the shaft by the 14th year in females, sixteenth in males. The distal epiphysis unites with the shaft in the 17th year in females, 18th in males.
MUSCLES
ANTERIOR COMPARTMENT
The anterior compartment contains the flexor muscles of the forearm which are arranged in superficial and deep groups. Chronic tendonitis of the common flexor tendon origin produces medial epicondylitis of the elbow, leading to pain and tenderness. It is a frequent complaint among golfers. A detailed account of the architectural properties of the muscles of the arm and forearm is given by Leiber et al (1992).
Superficial flexor compartment
Muscles of the superficial flexor compartment arise from the medial epicondyle of the humerus by a common tendon. They are pronator teres, flexor carpi radialis, palmaris longus, flexor digitorum superficialis, and flexor carpi ulnaris (Fig. 49.12). They have additional attachments to the antebrachial fascia near the elbow and to the septa that pass from this fascia between individual muscles.
Pronator teres
Pronator teres has humeral and ulna attachments (Fig. 49.3, Fig. 49.12, Fig. 49.13). The humeral head, the larger and more superficial of the two, arises just proximal to the medial epicondyle, from the common tendon of origin of the flexor muscles, from the intermuscular septum between it and flexor carpi radialis, and from antebrachial fascia. The smaller ulnar head springs from the medial side of the coronoid process of the ulna, distal to the attachment of flexor digitorum superficialis, and joins the humeral head at an acute angle. The muscle passes obliquely across the forearm to end in a flat tendon that is attached to a rough area midway along the lateral surface of the radial shaft at the ‘summit’ of its lateral curve. The coronoid attachment may be absent. Accessory slips may arise from a supracondylar process of the humerus, if it is present, or from biceps, brachialis or the medial intermuscular septum.
Flexor carpi radialis
Flexor carpi radialis lies medial to pronator teres, and arises from the medial epicondyle via the common flexor tendon, from the antebrachial fascia and from adjacent intermuscular septa (Fig. 49.12). Its fusiform belly ends, rather more than halfway to the wrist, in a long tendon which passes within a synovial sheath through a lateral canal, formed by the flexor retinaculum above and a groove on the trapezium beneath. It inserts on the palmar surface of the base of the second metacarpal, sending a slip to the third metacarpal. These distal attachments are hidden by the oblique head of adductor pollicis. The muscle rarely may be absent. It may have accessory slips from the biceps tendon, bicipital aponeurosis, coronoid process or radius. Distally it may also be attached to the flexor retinaculum, trapezium or fourth metacarpal.






