CHAPTER 205 Evaluation and Management of the Stridulous Child
Advances in medical technology impact the likely underlying diagnoses of modern-day stridor and its management.1 Developments in neonatal intensive care have seen improved neonatal survival and the associated challenges of the airway pathology seen in these children. Routine childhood immunization with the Haemophilus influenzae type B (HiB) vaccine has led to a precipitous decline in epiglottitis, making it a rarity. Improvements in endoscopic equipment have revolutionized the quality of optical images obtainable and captured for digital recording. It has also allowed for the development of endoscopic interventions in the compromised pediatric airway, many of which may now be used in combination to avoid tracheotomy or open airway surgery.
Definition and Physical Principles
Stridor is an audible respiratory noise derived from turbulent airflow due to narrowing or obstruction of the upper airway. Stridor may be inspiratory, biphasic, or expiratory in nature. It is classically a harsh sound, which can vary in quality from a squeak to a whistling noise. Stertor describes the snoring-like noise, which typically originates from nasopharyngeal or oropharyngeal obstruction. Clinically, however, the supraglottic larynx can occasionally produce this quality of noise. Obstruction from all levels of the airway should thus be considered when approaching the differential diagnoses of airway obstruction (Table 205-1).
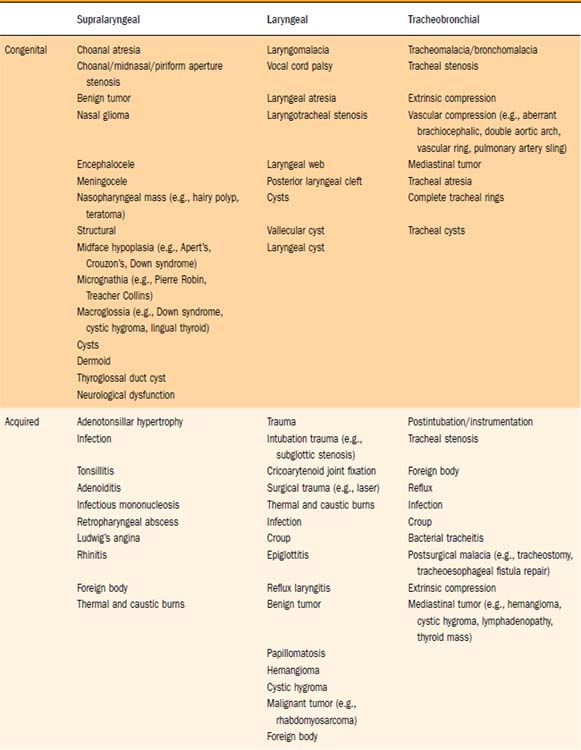
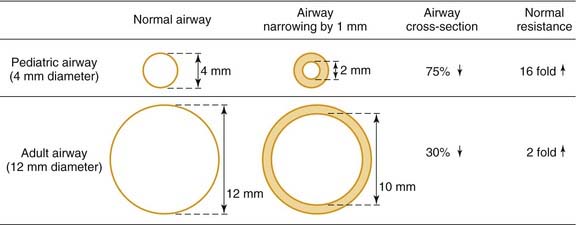
It is helpful to review the physical principles of tubular flow according to Poiseuille’s law, which states that Q = [πr4(P1-P2)]/8ηL; where Q is flow, r is radius, P is pressure, η is viscosity, and L is length of tube. From this law, resistance is inversely proportional to the radius to the fourth power. From a practical viewpoint, this explains why minor narrowing in a child’s airway is of much greater consequence than in an adult. For example, 1 mm of edema in a 4-mm diameter pediatric airway will reduce the cross-sectional area by 75% (16-fold increase in resistance), whereas in a 12-mm adult airway, the same 1 mm of edema reduces the airway area by just 30% (twofold increase in resistance) as demonstrated in Fig. 205-1.2
Assessment
Stridor may be characteristic of a particular pathology but is never diagnostic. The diagnosis can be confirmed with certainty only after endoscopy. However, the combination of a thorough history, examination, and investigation can in some conditions (e.g., mild laryngomalacia) provide sufficient diagnostic probability to avoid initial rigid endoscopy. Seventeen percent of infants with laryngomalacia have a synchronous lesion that may be contributing to their airway compromise.3 This may be missed without assessment via rigid endoscopy.
History
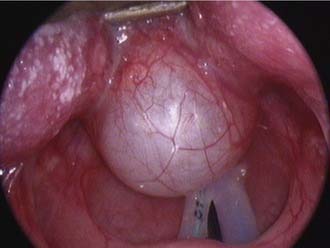
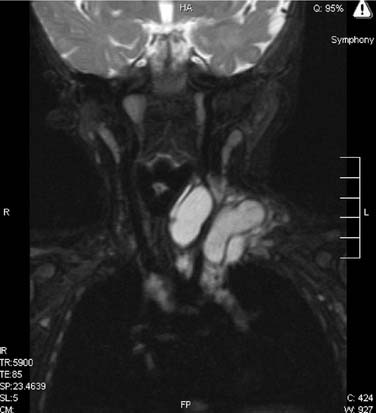
Features of the stridor, including the timing of onset, progression, variability, and presence of exacerbating or relieving factors should be carefully established. Stridor present from birth suggests an underlying anatomic cause. This generally denotes a fixed congenital narrowing such as a laryngeal web, subglottic stenosis, or tracheal narrowing.4 Dynamic conditions such as laryngomalacia typically become evident in the first few weeks of life, while congenital vocal cord palsy is also a common cause of neonatal stridor. A gradual increase in severity of stridor or airway compromise implies progressive obstruction. The obstruction may be luminal (as in a subglottic hemangioma) or extrinsic (as with a mediastinal mass or vascular anomaly). Alternatively over a longer period of time, increasing stridor may coincide with increased respiratory demands as the child becomes more active. Typically, laryngomalacia improves during rest or sleep but is worsened by crying, feeding, or physical activity. Airway obstruction associated with supine positioning may occur with supralaryngeal obstruction, such as micrognathia wherein there is associated airway obstruction by the tongue base. More rarely a pedunculated laryngeal mass, for example, a vallecular cyst, can give positional variation in the stridor as it is displaced in and out of the airway (Fig. 205-2). Improved airway obstruction with crying may occur in gross nasal obstruction such as bilateral choanal atresia.
Airway obstruction produces a number of associated symptoms (Table 205-2) that may be useful in formulating a differential diagnosis. Parents have often observed signs of increased respiratory work, including tracheal tug, subcostal recession, and suprasternal or sternal indrawing. Apneas with cyanosis may occur and parents often attempt resuscitation if these are severe. These episodes are typical of severe tracheobronchomalacia and are sometimes termed dying spells. The differential diagnosis includes underlying congenital cardiac disease, hence these episodes should be investigated further. Cough is typical of tracheoesophageal fistula and tracheomalacia, and raises the possibility of aspiration. Hoarseness suggests laryngeal pathology such as laryngeal papillomatosis (Fig. 205-3), whereas supralaryngeal pathology may give a muffled voice. Voice change may also occur in vocal cord palsy, although these children can also present with airway compromise and a normal voice.5,6 Tachypnea and dyspnea are not limited to upper airway obstruction, but a clear description of exertional dyspnea in an older child may provide a useful functional assessment of severity.
Table 205-2 Features of History and Examination in the Stridulous Child
| Symptoms | Signs |
|---|---|

The baby may feed slowly due to airway obstruction and “run out of breath” or “come up for air” during feeds. Bottle-fed babies may require thickened feeds or a “slow teat” (i.e., one with small holes). Uncomplicated slow feeding, although often a source of significant maternal anxiety, is not necessarily of concern in isolation. However, if there is failure to thrive and documented poor weight gain on the centile growth chart, further investigation and possible intervention should be considered. Laryngomalacia commonly gives rise to feeding difficulties but it is important to consider other causes. Choking episodes, documented aspiration, or recurrent chest infections may occur with vocal cord palsy, tracheoesophageal fistula, or rarely a laryngeal cleft (see Fig. 205-21). Gastroesophageal reflux is also common in infants with stridor and may exacerbate airway obstruction via edema.
The obstetric and perinatal histories are often relevant, especially if the child was born prematurely and required ventilation. Parents should be specifically asked about neonatal intubation. This history must be taken carefully because the passage of nasogastric tubes for feeding or nasal/oral mucous suctioning may be mistaken for intubation. Previous intubation places the child at an increased risk of acquired subglottic stenosis (see Fig. 205-13). If the child was recently intubated or is being assessed due to failed extubation, it is worthwhile to obtain details, including size of the endotracheal tube used in comparison to the predicted age-appropriate tube, presence of a leak during intubation, use of steroids at the time of extubation, and any previous history of failed extubations.
Other comorbidities may predispose to airway obstruction, for example, vocal cord palsy in Arnold-Chiari malformation or birth injury, neurologic disease giving rise to hypotonia, or iatrogenic injury following cardiac surgery. A previously diagnosed syndrome may alert the clinician to potential pathology that is recognized as a component of the syndrome, for example, laryngeal webs in velocardiofacial syndrome. Vascular malformations, congenital cardiac disease, or vascular anomalies may give extrinsic compression of the airway and subsequent tracheomalacia. Parents should be asked about the presence of any “birthmarks,” in that 50% of children with a subglottic hemangioma have a cutaneous lesion at the time of diagnosis (Fig. 205-4).7 There is a markedly increased risk for children with cutaneous hemangiomas in a “beard” distribution, with 63% having significant airway involvement (Fig. 205-5).8 The clinician should be particularly vigilant in assessing children with a history of recurrent episodes of laryngotracheitis or bronchiolitis that has been slow to settle. These children ought to be thoroughly assessed for an underlying source of airway obstruction that is being exacerbated by superimposed upper respiratory tract infection (Fig. 205-6).


Examination
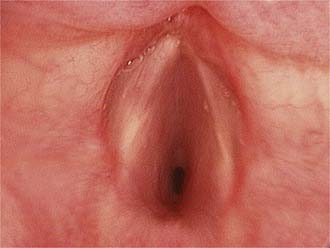
An overall assessment of the degree of respiratory distress and airway compromise should be expedited in the acute situation and a full examination completed if the child’s condition is stable (see Table 205-2). Observation of the child at rest in the parent’s arms provides an initial assessment of the degree of respiratory distress, the characteristics of any stridor, and whether the child appears systemically unwell. It also allows time to gain the child’s confidence before any further examination. A careful general examination is necessary to avoid missing subtle features of related syndromes or of other general pediatric disease. Syndromic features, if present, may suggest likely sources of airway obstruction associated with the particular syndrome, for example, micrognathia in Pierre Robin sequence, macroglossia in Beckwith-Wiedemann syndrome, or anterior glottic webs in velocardiofacial syndrome (Fig. 205-7).

Figure 205-7. Anterior glottic web presenting with stridor in a child with velocardiofacial syndrome.
Simple inspection of the child reveals valuable information regarding the work of breathing and degree of obstruction. Potential findings of increased respiratory work include suprasternal or sternal recession, subcostal indrawing, “see-saw” or paradoxical abdominal movement during respiration, nasal flaring, tracheal tug, anxiety, irritability, or evidence of fatigue. The amount of recession is a better indicator of the severity of airway compromise than the degree of stridor. Stridor can paradoxically become quieter and less apparent as the obstruction worsens due to the diminishing airflow and may be a sign of impending respiratory arrest. Pallor and subsequent cyanosis are late events in pediatric patients and no comfort should be taken from the fact that a child still appears pink. Children may position themselves to optimize their own airway as is classically described in epiglottitis, where children prefer to sit upright with their head in a “sniffing” position. Pectus excavatum may be seen in children with chronic airway obstruction due to negative intrathoracic pressure in their highly compliant rib cage.2
Inspiratory stridor typically occurs due to obstruction at the level of the supraglottis or glottis. Obstruction arising in the bronchi or lower trachea classically produces an expiratory stridor or prolongation of the expiratory phase. Biphasic stridor can occur with obstruction anywhere in the laryngotracheobronchial tree but is classically associated with either upper tracheal or subglottic pathology where it is attributed to the fixed luminal diameter of the cricoid. The characteristic sound of stridor, even in a common condition such as laryngomalacia,9 is so variable as to be of little diagnostic use in isolation. Laryngomalacia has been traditionally described as having stridor that is of a musical quality, while stridor in vocal cord palsy has a breathy quality, viral laryngotracheitis has a barking cough and tracheomalacia has a brassy cough. It is important to recognize that these descriptions are highly subjective and their assessment is not reliably reproducible.
Radiology
Soft tissue lateral neck x-ray examination demonstrates the airway outline from the nasopharynx to the subglottis. Posterior-anterior chest x-ray study shows the lung fields and mediastinum. Persistent air trapping may be demonstrated on the side of a bronchial foreign body in inspiratory/expiratory views. A decubitus view may be useful in young children, where normally the dependent lung deflates.10 A Cincinnati (high-kilovoltage filter) view enhances the tracheal air column while de-emphasizing bony cervical spine to demonstrate the major airways. These x-ray techniques may be useful as screening investigations (Fig. 205-8).11,12 Careful consideration of the stability of the child’s airway is mandatory and radiology should not be undertaken if there is any potential for acute airway deterioration. Policy for suspected epiglottitis differs between centers; however, the result of the x-ray study may not influence management13 and may be associated with significant risk to the child. Further imaging should be performed according to the endoscopy findings.

Videofluoroscopy is an excellent way of demonstrating tracheomalacia and can be combined with a contrast swallow to exclude vascular compression,14,15 tracheoesophageal fistula, or aspiration. It may demonstrate diaphragmatic immobility on the side of a foreign body airway obstruction. Bronchograms using safe nonionic contrast media are useful for outlining the luminal surface of the lower airway, demonstrating tracheobronchial stenosis and malacia. Opening pressures of the collapsed bronchi and lower trachea can also be measured to determine the level of airway support needed. Computed tomography (CT) and magnetic resonance imaging (MRI)12,16,17 continue to lack sensitivity in assessing airway stenoses and cannot replace endoscopic assessment. They are useful in demonstrating vascular anomalies and extrinsic compression of the airway (Fig. 205-9). Virtual endoscopy uses radiologic data to create computer simulations that may be viewed as one would conventional endoscopy. Helical CT with multiplanar reconstruction provides three-dimensional images, which are used in real time to simulate endoscopy views. It is noninvasive and allows retrograde luminal airway views. Although it demonstrates some fixed airway stenoses, it is not helpful in detecting obstruction during dynamic movement as occurs in tracheomalacia or vocal cord palsy. There is also a lack of detail, with airway pathology such as glottic webs being poorly demonstrated.18
Other Investigations
Vocal cord ultrasound can be used, with experience, to demonstrate vocal cord palsy to complement the endoscopic findings.19 The role of laryngeal EMG in the management of vocal cord immobility is yet to be fully defined.20 Airway obstruction that worsens during sleep is usually a feature of pharyngeal obstruction, such as adenotonsillar obstruction or craniofacial anomaly. Laryngotracheal pathology at any level including laryngomalacia may, however, occasionally worsen during sleep, thus requiring sleep study investigation.21 Pediatric lung function tests are seldom used because of compliance and cooperation issues. Flow volume loops22 may help localize the site of obstruction and other tests such as peak flows or ventilation-perfusion scans may be used upon the advice of a pulmonologist. Gastroesophageal reflux23–26 is not discussed in detail in this chapter but can be investigated via double probe pH studies, contrast studies, milk scan, or esophagoscopy with lower esophageal biopsy. Echocardiography detects congenital heart disease but does not demonstrate all abnormal vasculature, thus it cannot be used to exclude vascular anomalies.
Endoscopy
Pediatric airway endoscopy requires a full range of specialized pediatric endoscopy equipment and an experienced team. An inadequate evaluation needs to be repeated, and referral to an experienced center should be made as required to ensure a single comprehensive and definitive evaluation. A systematic approach provides a diagnosis in most cases.27
Flexible Endoscopy in the Office or Ward
The introduction of ultrathin endoscopes28 in a range of diameters with good optics has allowed even neonates to undergo endoscopy without the need for a general anesthetic. This is usually considered a screening procedure, in that the view of the larynx may be suboptimal. Rigid endoscopy of the airway is superior in examining the airway for structural abnormalities. Flexible endoscopy is useful in assessing the dynamic airway for vocal cord movement or features of laryngomalacia. A systematic approach must be adopted, observing first the nasal cavity followed by the postnasal space, oropharynx, supraglottis, and glottis during dynamic respiration and phonation. It is difficult to obtain good views of the subglottis. This is purely a diagnostic procedure, with no opportunity for therapeutic procedures, in contrast to a rigid laryngotracheobronchoscopy. Flexible endoscopy under sedation in an endoscopy suite is widely practiced by pediatricians and pulmonologists29–31 and is used by otolaryngologists as an adjunct to rigid endoscopy.32 Rigid endoscopy is helpful if the diagnosis remains unclear despite flexible endoscopy, if there is clinical suspicion of a second airway lesion, or if subglottic/tracheal or bronchial pathology is suspected.
Laryngotracheobronchoscopy
Laryngotracheobronchoscopy33 is the gold standard in the evaluation of the stridulous child. It enables a thorough assessment to be performed while the airway is maintained and allows findings to be visually recorded for future reference. The airway may be formally sized to grade any narrowing. It also may incorporate therapeutic procedures, including foreign body removal or the endoscopic management of airway pathology. It requires an experienced team skilled in airway assessment, including the surgeon, anesthetist, and nursing assistant, who work closely to ensure an optimal and safe examination. The use of a video is essential to facilitate training and allows the anesthetist and nurse to follow the procedure and status of the airway on the monitor.
It is vital that accurate records are kept in a standardized form within a department.34 Digital prints provide a valid record of static conditions while video clips record dynamic findings. Digital images and video recordings should be saved and archived. This provides an invaluable source of information for sequential clinical comparisons, teaching, and medicolegal purposes.
Anesthetic Considerations
This procedure requires a cooperative approach to airway management with both the anesthetic team and surgeon sharing the control of the airway. The use of atropine premedication provides a dry surgical field and improves the efficacy of topical anesthesia. It is most effective via intramuscular injection. Anesthesia is often induced using slow masked inhalational anaesthesia. Halothane is a volatile agent that has been traditionally used and is nonirritating to the airway, allowing for smooth maintenance of anesthesia during instrumentation of the airway. Halothane is now difficult to obtain and other inhalational agents such as isoflurane, sevoflurane, and intravenous agents are being used. Sevoflurane35 is also nonirritating, rapid in onset, and allows rapid delivery of high concentrations. Topical lidocaine is applied to the airway to minimize airway stimulation during the procedure and helps avoid laryngospasm. Lidocaine dose needs to be carefully measured to avoid overdosage.36,37
Anesthetic practice varies between centers but most units use spontaneous respiration for pediatric patients rather than paralysis and jet ventilation simulating normal respiration. Jet ventilation prevents coughing or gagging38–40 but requires pressures above physiologic levels38,41 with an associated risk of pneumothorax in neonates and smaller children. Dynamic conditions such as malacia and cord palsy cannot be identified. Apneic endoscopy is also possible after initial hyperventilation with 100% oxygen, although progressive hypoxemia and hypercarbia limit the operating time and condition of the patient.42
A laryngeal mask43 may be useful for fiberoptic bronchoscopy particularly if the patient is difficult to intubate due to mandibular hypoplasia.
Operative Technique
A suspension laryngoscope and microscope are traditionally used to examine the larynx, with a ventilating bronchoscope to examine the tracheobronchial tree (Fig. 205-10). Rigid telescopes provide excellent images and many centers now perform the assessment using a telescope, with digital images recorded at each anatomic level. High-quality images may be captured via the use of a wide Storz photographic telescope. A 4-mm rigid telescope should provide adequate images for data records, provided there is careful focusing and appropriate camera settings to ensure optimal captured images. For routine examination, the telescope and camera can be held in the left hand with a probe used in the right while the laryngoscope is in suspension. The microscope is used if there is to be manipulation of the airway requiring both hands of the operating surgeon. Differing techniques are adopted, according to individual departmental preferences. The procedure may be combined with rigid esophagoscopy, according to departmental protocols.

Preparation and Positioning
It is essential to anticipate equipment requirements so all equipment can be checked and prepared before commencement. A range of Hopkins rod telescopes should be available, which includes all lengths and diameters that may be required, so the endoscopist is fully prepared for all eventualities. Charts that predict age-appropriate sizes of bronchoscopes should be consulted and be readily available in the operating room.44 The appropriate bronchoscope needs to be checked and assembled and at least one size smaller must be on hand. A 30-degree telescope may be used to enable assessment of the supraglottis without splinting. It may also assist assessment of an anteriorly placed larynx. A microscope should be available with the 400-mm lens to be used with standard laryngeal instruments. A 350-mm lens may be useful in small neonates by “bringing the patient closer” to allow easier manipulation of larynx.
Microlaryngoscopy Technique
A suspension straight-blade laryngoscope is gently inserted while assessing the overall appearance of the laryngopharynx, taking care to protect the teeth, lips, and oral mucosa while keeping the tongue midline to provide a well-centered view. The laryngoscope is placed in the vallecula and the epiglottis is carefully lifted forward. An overall assessment of the larynx can be made while an endotracheal tube is in situ and while providing a degree of stability, particularly in a compromised pediatric airway. Removal of the endotracheal tube allows a superior view and a probe may be used to independently palpate the arytenoids to assess the mobility of the cricoarytenoid joints and any limitation in joint movement. Absence of independent arytenoid movement on palpation is indicative of interarytenoid scarring. A posterior laryngeal cleft should be excluded by passing the probe between the arytenoids to allow comparison of the inferior limit of the interarytenoid groove with the posterior commissure. The subglottis should also be inspected from above. Topical decongestion and vasoconstriction of the airway may be helpful, particularly in the presence of low-grade inflammation or edema. Any airway narrowing should be formally sized. The largest endotracheal tube that permits a leak at less than 30 cm H2O of pressure provides a measure of the airway diameter. Subglottic stenosis may then be graded using the Cotton-Myer grading system,45 thus allowing reproducible assessment of the stenosis and aiding in treatment selection. If there is airway compromise or instability, assessment time may be limited. It is thus essential to be prepared to move ahead with bronchoscopy at any stage.
Bronchoscopy Technique
Traditionally, a ventilating bronchoscope (Fig. 205-11) has been used to assess the distal airway, which provides a means of actively ventilating the patient during the procedure, if required. An age-appropriate sized bronchoscope is used unless stenosis is suspected. A smaller-diameter rigid Hopkins rod telescope can be used as an alternative to examine the airway in a spontaneously breathing child, particularly if there is significant subglottic stenosis. The rigid telescope may reduce local airway trauma and lessen airway splinting, while allowing the distal airway to be visualized.







