Dyspnea
Perspective
Dyspnea is the term applied to the sensation of breathlessness and the patient’s reaction to that sensation. It is an uncomfortable awareness of breathing difficulties that in the extreme manifests as “air hunger.” Dyspnea is often ill defined by patients, who may describe the feeling as shortness of breath, chest tightness, or difficulty breathing. Dyspnea results from a variety of conditions, ranging from nonurgent to life-threatening. Neither the clinical severity nor the patient’s perception correlates well with the seriousness of underlying pathology and may be affected by emotions, behavioral and cultural influences, and external stimuli.1,2
The following terms may be used in the assessment of the dyspneic patient:
Tachypnea: A respiratory rate greater than normal. Normal rates range from 44 cycles/min in a newborn to 14 to 18 cycles/min in adults.
Hyperpnea: Greater than normal minute ventilation to meet metabolic requirements.
Hyperventilation: A minute ventilation (determined by respiratory rate and tidal volume) that exceeds metabolic demand. Arterial blood gases (ABGs) characteristically show a normal partial pressure of oxygen (PO2) with an uncompensated respiratory alkalosis (low partial pressure of carbon dioxide [PCO2] and elevated pH).
Dyspnea on exertion: Dyspnea provoked by physical effort or exertion. It often is quantified in simple terms, such as the number of stairs or number of blocks a patient can manage before the onset of dyspnea.
Orthopnea: Dyspnea in a recumbent position. It usually is measured in number of pillows the patient uses to lie in bed (e.g., two-pillow orthopnea).
Paroxysmal nocturnal dyspnea: Sudden onset of dyspnea occurring while reclining at night, usually related to the presence of congestive heart failure.
Pathophysiology
The actual mechanisms responsible for dyspnea are unknown. Normal breathing is controlled both centrally by the respiratory control center in the medulla oblongata and peripherally by chemoreceptors located near the carotid bodies, and mechanoreceptors in the diaphragm and skeletal muscles.3 Any imbalance among these sites is perceived as dyspnea. This imbalance generally results from ventilatory demand being greater than capacity.4
Diagnostic Approach
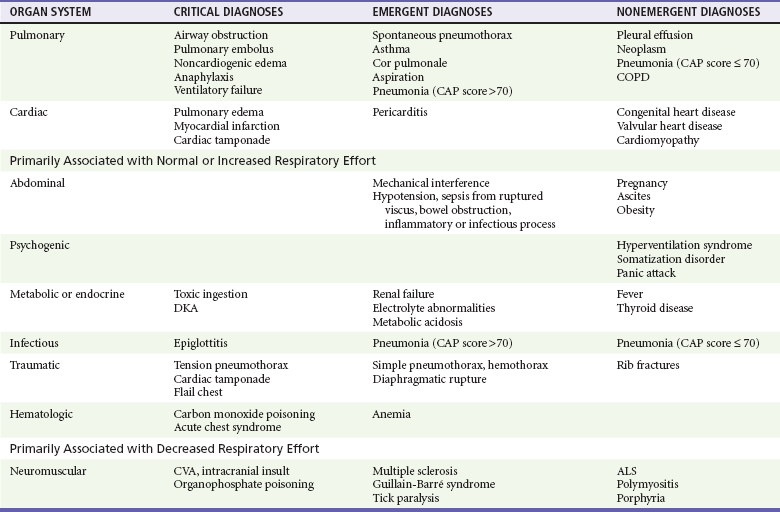
Dyspnea is subjective and has many different potential causes. The differential diagnosis can be divided into acute and chronic causes, of which many are pulmonary. Other causes include cardiac, metabolic, infectious, neuromuscular, traumatic, and hematologic conditions (Table 25-1).
Pivotal Findings
Duration of Dyspnea.: Chronic or progressive dyspnea usually denotes primary cardiac or pulmonary disease.5 Acute dyspneic spells may result from asthma exacerbation; infection; pulmonary embolus; intermittent cardiac dysfunction; psychogenic causes; or inhalation of irritants, allergens, or foreign bodies.
Onset of Dyspnea.: Sudden onset of dyspnea should lead to consideration of pulmonary embolism (PE) or spontaneous pneumothorax. Dyspnea that builds slowly over hours or days may represent a flare of asthma or COPD; pneumonia; recurrent, small pulmonary emboli; congestive heart failure; or malignancy.
Positional Changes.: Orthopnea can result from left-sided heart failure, COPD, or neuromuscular disorders. One of the earliest symptoms seen in patients with diaphragmatic weakness from neuromuscular disease is orthopnea.6 Paroxysmal nocturnal dyspnea is most common in patients with left-sided heart failure5 but also occurs in COPD. Exertional dyspnea commonly is associated with COPD but also can be seen with poor cardiac reserve and abdominal loading. Abdominal loading, caused by ascites, obesity, or pregnancy, leads to elevation of the diaphragm, resulting in less effective ventilation and dyspnea.
Symptoms
Patient descriptions of dyspnea vary significantly and generally correlate poorly with severity. Fever suggests an infectious cause. Anxiety or overwhelming fear, particularly if it precedes the onset of dyspnea, may point to panic attack or psychogenic dyspnea, if no organic cause can be isolated. PE or myocardial infarction may cause isolated dyspnea with or without associated chest pain, particularly if the pain is constant, dull, or visceral.7 If the pain is sharp and worsened by deep breathing but not by movement, pleural effusion, pleurisy, or pleural irritation from pneumonia or PE are possible. Spontaneous pneumothorax also may produce sharp pain with deep breathing that is not worsened by movement.
Signs
Physical signs in dyspneic patients may be consistent with specific illnesses (Table 25-2). Physical findings found in specific diseases also can be grouped as presenting patterns (Table 25-3).
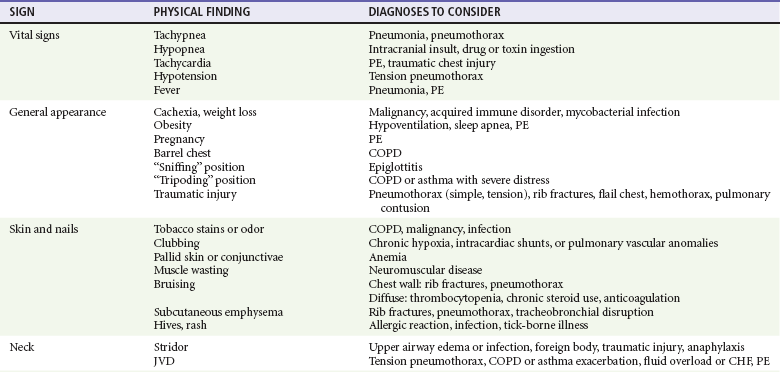
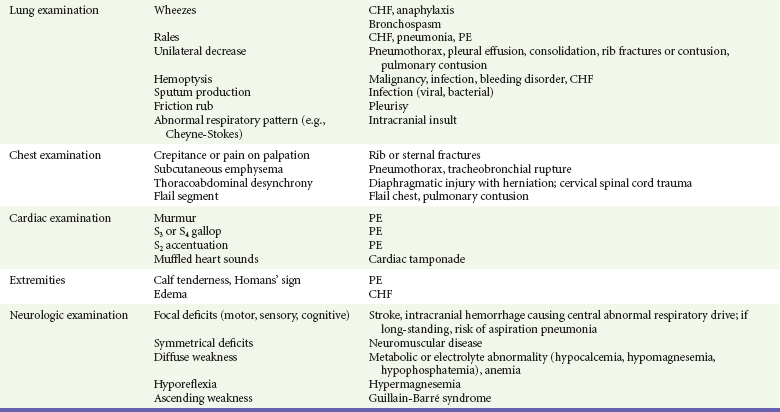
Table 25-3
Diagnostic Table: Patterns of Diseases Often Resulting in Dyspnea


