Contemporary issues and theories of motor control, motor learning, and neuroplasticity
MARGARET L. ROLLER, PT, MS, DPT, ROLANDO T. LAZARO, PT, PhD, DPT, GCS, NANCY N. BYL, PT, MPH, PhD, FAPTA and DARCY A. UMPHRED, PT, PhD, FAPTA
After reading this chapter the student or therapist will be able to:
1. Identify the evolution of motor control theories and discuss the utility of current theory in clinical practice.
2. Identify body structures and functions that contribute to the control of human posture and movement.
3. Relate the cognitive, associative, and autonomous stages of motor learning to behavior and skill performance.
4. Describe the variety of practice conditions that may be used to enhance motor learning within a practice session.
5. Apply motor learning variables related to person, task, and environment within the therapeutic setting.
6. Discuss neuroplasticity theories that explain how the nervous system adapts to demands placed on learning and performance.
7. Discuss the relationship among motor control, motor learning, and neuroplasticity in the production of functional movement behaviors.
This chapter introduces the reader to basic concepts of motor control, motor learning, and neuroplasticity. Figures and tables are provided within each section to emphasize and summarize concepts. A patient case example is used to illustrate concepts in this chapter as they apply to the evaluation and management of people with neurological conditions. This chapter provides a foundation for chapters in Section II: Rehabilitation Management of Clients with Neurological System Pathology, and acts as a foundation for interacting with and treating patients in any clinical setting.
Motor control
Motor control is defined as “the systematic transmission of nerve impulses from the motor cortex to motor units, resulting in coordinated contractions of muscles.”1
Theories and models of motor control
We begin this section with a summary and historical perspective of motor control theories (Table 4-1). The control of human movement has been described in many different ways. The production of reflexive, automatic, adaptive, and voluntary movements and the performance of efficient, coordinated, goal-directed movement patterns involve multiple body systems (input, output, and central processing) and multiple levels within the nervous system. Each model of motor control that is discussed in this section has both merit and disadvantage in its ability to supply a comprehensive picture of motor behavior. These theories serve as a basis for predicting motor responses during patient examination and treatment. They help explain motor skill performance, potential, constraints, limitations, and deficits. They allow the clinician to (1) identify problems in motor performance, (2) develop treatment strategies to help clients remediate performance problems, and (3) evaluate the effectiveness of intervention strategies employed in the clinic. Selecting and using an appropriate model of motor control is important for the analysis and treatment of clients with dysfunctions of posture and movement. As long as the environment and task demands affect changes in the CNS and the individual has the desire to learn, the adaptable nervous system will continue to learn, modify, and adapt motor plans throughout life.
TABLE 4-1 
| MOTOR CONTROL THEORY | AUTHOR AND DATE | PREMISE |
| Reflex Theory | Sherrington 1906244 | Movement is controlled by stimulus-response. Reflexes are combined into actions that create behavior. |
| Hierarchical Theories | Adams 1971245 | Cortical centers control movement in a top-down manner throughout the nervous system.Closed-loop mode: sensory feedback is needed and used to control the movement. Open-loop mode: movements are preprogrammed and no feedback is used. |
| Dynamical Systems Theory | Bernstein 196710Turvey 1977246 Kelso and Tuller 1984247 Thelen 1987248 |
Movement emerges to control degrees of freedom.Patterns of movements self-organize within the characteristics of environmental conditions and the existing body systems of the individual. Functional synergies are developed naturally through practice and experience and help solve the problem of coordinating multiple muscles and joint movements at once. |
| Motor Program Theory | Schmidt 1976249 | Adaptive, flexible motor programs (MPs) and generalized motor programs (GMPs) exist to control actions that have common characteristics. |
| Ecological Theories | Gibson and Pick 2000250 | The person, the task, and the environment interact to influence motor behavior and learning. The interaction of the person with any given environment provides perceptual information used to control movement. The motivation to solve problems to accomplish a desired movement task goal facilitates learning. |
| Systems Model | Shumway-Cook 200735 | Multiple body systems overlap to activate synergies for the production of movements that are organized around functional goals. Considers interaction of the person with the environment. |
Motor programs and central pattern generators
A motor program (MP) is a learned behavioral pattern defined as a neural network that can produce rhythmic output patterns with or without sensory input or central control.2 MPs are sets of movement commands, or “rules,” that define the details of skilled motor actions. An MP defines the specific muscles that are needed, the order of muscle activation, and the force, timing, sequence, and duration of muscle contractions. MPs help control the degrees of freedom of interacting body structures, and the number of ways each individual component acts. A generalized motor program (GMP) defines a pattern of movement, rather than every individual aspect of a movement. GMPs allow for the adjustment, flexibility, and adaptation of movement features according to environmental demands. The existence of MPs and GMPs is a generally accepted concept; however, hard evidence that an MP or a GMP exists has yet to be found. Advancements in brain imaging techniques may substantiate this theory in the future.2,3
In contrast to MPs, a central pattern generator (CPG) is a genetically predetermined movement pattern.4 CPGs exist as neural networks within the CNS and have the capability of producing rhythmic, patterned outputs resembling normal movement. These movements have the capability of occurring without sensory feedback inputs or descending motor inputs. Two characteristic signs of CPGs are that they result in the repetition of movements in a rhythmic manner and that the system returns to its starting condition when the process ceases.5 Both MPs and CPGs contribute to the development, refinement, production, and recovery of motor control throughout life.
Body structures and functions that contribute to the control of human posture and movement
Role of sensory information in motor control
Sensory information is necessary during the acquisition phase of learning a new motor skill and is useful for controlling movements during the execution of the motor plan.6–8 However, sensory information is not always necessary when performing well-learned motor behaviors in a stable and familiar context.6,7 Rothwell and colleagues7 studied a man with severe sensory neuropathy in the upper extremity. He could write sentences with his eyes closed and drive a car with a manual transmission without watching the gear shift. He did, however, have difficulty with fine motor tasks such as buttoning his shirt and using a knife and fork to eat when denied visual information. The importance of sensory information must be weighed by the individual, unconsciously filtering and choosing appropriate and accurate sensory inputs to use to meet the movement goal.
Sensory experiences and learning alter sensory representations, or cortical “maps,” in the primary somatosensory, visual, and auditory areas of the brain. Training, as well as use and disuse of sensory information, has the potential to drive long-term structural changes in the CNS, including the formation, removal, and remodeling of synapses and dendritic connections in the cortex. This process of cortical plasticity is complex and involves multiple cellular and synaptic mechanisms.9 Plasticity in the nervous system is discussed further in the third section of this chapter.
Coordination
The movement plan is customized by communications among the frontal lobes, basal ganglia, and cerebellum, with functional connections through the brain stem and thalamus. During this process specific details of the plan are determined. Postural tone, coactivation, and timing of trunk muscle firing are set for proximal stability, balance, and postural control. Force, timing, and tone of limb synergies are set to allow for smooth, coordinated movements that are accurate in direction of trajectory, order, and sequence. The balance between agonist and antagonist muscle activity is determined so that fine distal movements are precise and skilled. This process is complicated by the number of possible combinations of musculoskeletal elements. The CNS must solve this “degrees of freedom” problem so that rapid execution of the goal-directed movement can proceed and reliably meet the desired outcome.10 Once these movement details are complete the motor plan is executed by the primary motor area in the precentral gyrus of the frontal lobe.
Adaptation
Adaptation is the process of using sensory inputs from multiple systems to adapt motor plans, decrease performance errors, and predict or estimate consequences of movement choices. The goal of adaptation is the production of consistently effective and efficient skilled motor actions. When all possible body systems and environmental conditions are considered in the motor control process, it is easy to understand why there is often a mismatch between the movement plan that is chosen and how it is actually executed. Errors in movements occur and cause problems that the nervous system must solve in order to deliver effective, efficient, accurate plans that meet the task goal. To solve this problem the CNS creates an internal representation of the body and the surrounding world. This acts as a model that can be adapted and changed in the presence of varying environmental demands. It allows for the ability to predict and estimate the differences between similar situations. This ability is learned by practicing various task configurations in real-life environments. Without experience, accurate movement patterns that consistently meet desired task goals are difficult to achieve.11
Anticipatory control
Anticipatory control of posture and postural adjustments stabilizes the body by minimizing displacement of the center of gravity. Anticipatory control involves motor plans that are programmed to act in advance of movement. A comparison between incoming sensory information and knowledge of prior movement successes and failures enables the system to choose the appropriate course of action.3
Flexibility
A person should have enough flexibility in performance to vary the details of a simple or complex motor plan to meet the challenge presented by any given environmental context. This is a beneficial characteristic of motor control. When considering postural control, for example, a person will typically display a random sway pattern during standing that may ensure continuous, dynamic sensory inputs to multiple sensory systems.12 The person is constantly adjusting posture and position to meet the demand of standing upright (earth vertical), as well as to seek information from the environment. Rhythmic, oscillating, or stereotypical sway patterns that are unidirectional in nature are not considered flexible and are not as readily adaptable to changes in the environment. Lack of flexibility or randomness in postural sway may actually render the person at greater risk for loss of balance and falls.
Control of voluntary movement
Table 4-2 shows the body system processes involved in motor control, their actions, and the body structures included. The following section explains these processes in more detail.
TABLE 4-2 
| PROCESS | ACTION | BODY STRUCTURES INVOLVED |
| Sensation | Sensory information, feedback from exteroceptors and proprioceptors | Peripheral afferent neurons, brain stem, cerebellum, thalamus, sensory receiving areas in the parietal, occipital, and temporal lobes |
| Perception | Combining, comparing, and filtering sensory inputs | Brain stem, thalamus, sensory association areas in the parietal, occipital, visual, and temporal lobes |
| Choice of movement plan | Use of the perceptual map to access the appropriate motor plan | Association areas, frontal lobe, basal ganglia |
| Coordination | Determining the details of the plan including force, timing, tone, direction, and extent of the movement of postural and limb synergies and actions | Frontal lobe, basal ganglia, cerebellum, thalamus |
| Execution | Execution of the motor plan | Corticospinal and corticobulbar tract systems, brain stem motor nuclei, and alpha and gamma motor neurons |
| Adaptation | Compare movement with the motor plan and adjust the plan during performance | Spinal neural networks, cerebellum |
Role of the cerebellum
The primary roles of the cerebellum are to maintain posture and balance during static and dynamic tasks and to coordinate movements before execution and during performance. The cerebellum processes multiple neural signals from (1) motor areas of the cerebral cortex for motor planning, (2) sensory tract systems (dorsal spinal cerebellar tract, ventral spinal cerebellar tract) from muscle and joint receptors for proprioceptive and kinesthetic sense information resulting from movement performance, and (3) vestibular system information for the regulation of upright control and balance at rest and during movements. It compares motor plan signals driven by the cortex with what is received from muscles and joints in the periphery and makes necessary adjustments and adaptations to achieve the intended coordinated movement sequence. Movements that are frequently repeated “instructions” are stored in the cerebellum as procedural memory traces. This increases the efficiency of its role in coordinating movement. The cerebellum also plays a role in function of the reticular activating system (RAS). The RAS network exists in the brain stem tegmentum and consists of a network of nerve cells that maintain consciousness in humans and help people focus attention and block out distractions that may affect motor performance. Damage to the cerebellum, its tract systems, or its structure creates problems of movement coordination, not execution or choice of which program to run. The cerebellum also plays a role in language, attention, and mental imagery functions that are not considered to take place in motor areas of the cerebral cortex (see Table 4-2).
The cerebellum plays four important roles in motor control13:
1. Feed-forward processing: The cerebellum receives neural signals, processes them in a sequential order, and sends information out, providing a rapid response to any incoming information. It is not designed to act like the cerebral cortex and does not have the capability of generating self-sustaining neural patterns.
2. Divergence and convergence: The cerebellum receives a great number of inputs from multiple body structures, processes this information extensively through a structured internal network, and sends the results out through a limited number of output cells.
3. Modularity: The cerebellum is functionally divided into independent modules—hundreds to thousands—all with different inputs and outputs. Each module appears to function independently, although they each share neurons with the inferior olives, Purkinje cells, mossy and parallel fibers, and deep cerebellar nuclei.
4. Plasticity: Synapses within the cerebellar system (between parallel fibers and Purkinje cells, and synapses between mossy fibers and deep nuclear cells) are susceptible to modification of their output strength. The influence of input on nuclear cells is adjustable, which gives great flexibility to adjust and fine-tune the relationship between cerebellar inputs and outputs.
Role of the basal ganglia
The basal ganglia are a collection of nuclei located in the forebrain and midbrain and consisting of the globus pallidus, putamen, caudate nucleus, substantia nigra, and subthalamic nuclei. It has primary functions in motor control and motor learning. It plays a role in deciding which motor plan or behavior to execute at any given time. It has connections to the limbic system and is therefore believed to be involved in “reward learning.” It plays a key role in eye movements through midbrain connections with the superior colliculus and helps to regulate postural tone as a basis for the control of body positions, preparedness, and central set. Refer to Chapter 20 for additional information on the basal ganglia.
Information processing
The processing of information through the sensory input, motor output, and central integrative structures occurs by various methods to produce movement behaviors. These methods allow us to deal with the temporal and spatial components necessary for coordinated motor output and allow us to anticipate so that a response pattern may be prepared in advance. Serial processing is a specific, sequential order of processing of information (Figure 4-1) through various centers. Information proceeds lockstep through each center. Parallel processing is processing of information that can be used for more than one activity by more than one center simultaneously or nearly simultaneously. A third and more flexible type of processing of information is parallel-distributed processing.14 This type of processing combines the best attributes of serial and parallel processing. When the situation demands serial processing, this type of activity occurs. At other times parallel processing is the mode of choice. For optimal processing of intrinsic and extrinsic sensory information by various regions of the brain, a combination of both serial and parallel processing is the most efficient mode. The type of processing depends on the constraints of the situation. For example, maintaining balance after an unexpected external perturbation requires rapid processing, whereas learning to voluntarily shift the center of gravity to the limits of stability requires a different combination of processing modes.
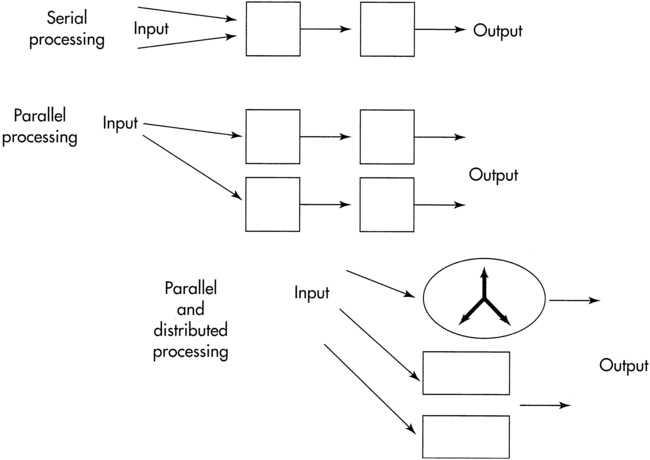
 Methods of information processing.
Methods of information processing.Movement patterns arising from self-organizing subsystems
Coordinated movement patterns are developed and refined via dynamic interaction among body systems and subsystems in response to internal and external constraints. Movement patterns used to accomplish a goal are contextually appropriate and arise as an emergent property of subsystem interaction. Several principles relate to self-organizing systems: reciprocity, distributed function, consensus, and emergent properties.15
Reciprocity implies information flow between two or more neural networks. These networks can represent specific brain centers, for example, the cerebellum and basal ganglia (Figure 4-2). Alternatively, the neural networks can be interacting neuronal clusters located within a single center, for example, the basal ganglia. One model to demonstrate reciprocity is the basal ganglia regulation of motor behavior through direct and indirect pathways to cortical areas. The more direct pathway from the putamen to the globus pallidus internal segment provides net inhibitory effects. The more indirect pathway from the putamen through the globus pallidus external segment and subthalamic nucleus provides a net excitatory effect on the globus pallidus internal segment. Alteration of the balance between these pathways is postulated to produce motor dysfunction.16,17 An abnormally decreased outflow from the basal ganglia is postulated to produce involuntary motor patterns, which produce excessive motion such as chorea, hemiballism, or nonintentional tremor. Alternatively, an abnormally increased outflow from the basal ganglia is postulated to produce a paucity of motions, as seen in the rigidity observed in individuals with Parkinson disease (see Chapter 20).
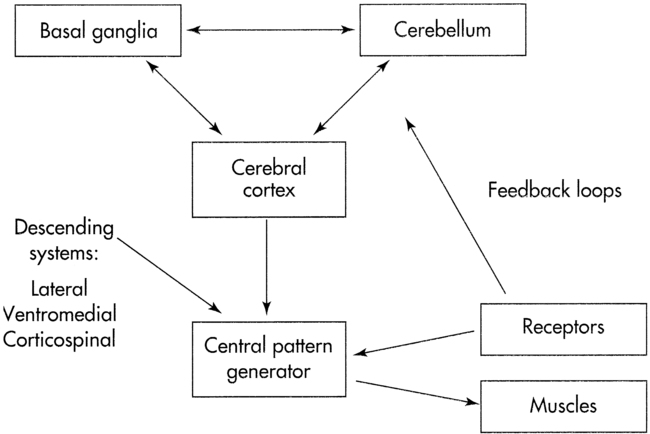
 Systems model of motor control.
Systems model of motor control.Distributed function presupposes that a single center or neural network has more than one function. The concept also implies that several centers share the same function. For example, a center may serve as the coordinating unit of an activity in one task and may serve as a pattern generator or oscillator to maintain the activity in another task. An advantage of distributing function among groups of neurons or centers is to provide centers with overlapping or redundant functions. Neuroscientists believe such redundancy is a safety feature. If a neuronal lesion occurs, other centers can assume critical functional roles, thereby producing recovery from CNS dysfunction.18–22
Emergent properties may be understood by the adage “the whole is greater than the sum of its parts.” This concept implies that brain centers, not a single brain center, work together to produce movement. An example of the emergent properties concept is continuous repetitive activity (oscillation). In Figure 4-3, A, a hierarchy is represented by three neurons arranged in tandem. The last neuron ends on a responder. If a single stimulus activates this network, a single response occurs. What is the response if the neurons are arranged so that the third neuron sends a collateral branch to the first neuron in addition to the ending on the responder? In this case (Figure 4-3, B), a single stimulus activates neuron No. 1, which in turn activates neurons No. 2 and No. 3, causing a response as well as reactivating neuron No. 1. This neuronal arrangement produces a series of responses rather than a single response. This process is also termed endogenous activity.
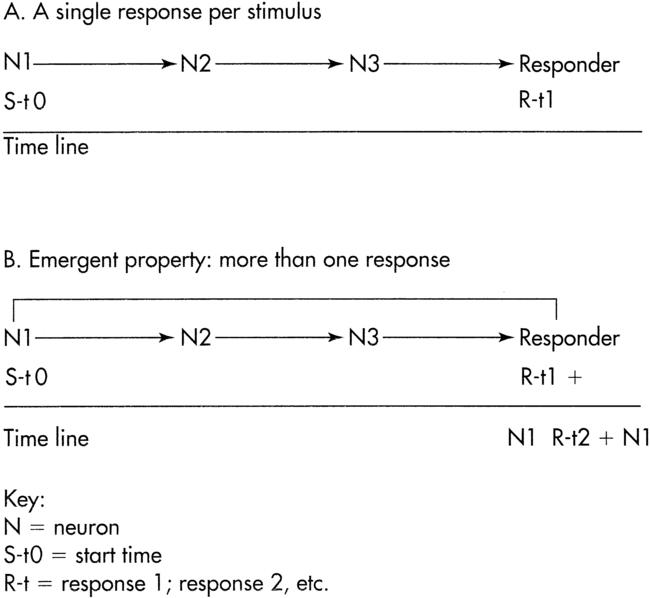
 Emergent property.
Emergent property.Controlling the degrees of freedom
Combinations of muscle and joint action permit a large number of degrees of freedom that contribute to movement. A system with a large number of degrees of freedom is called a high-dimensional system. For a contextually appropriate movement to occur, the number of degrees of freedom needs to be constrained. Bernstein10 suggested that the number of degrees of freedom could be reduced by muscles working in synergies, that is, coupling muscles and joints of a limb to produce functional patterns of movement. The functional unit of motor behavior is then a synergy. Synergies help to reduce the degrees of freedom, transforming a high-dimensional system into a low-dimensional system. For example, a step is considered to be a functional synergy pattern for the lower extremity. Linking together stepping synergies with the functional synergies of other limbs creates locomotion (interlimb coordination).
Functional synergy implies that muscles are activated in an appropriate sequence and with appropriate force, timing, and directional components. These components can be represented as fixed or “relative” ratios, and the control comes from input given to the cerebellum from higher centers in the brain and the peripheral or spinal system and from prior learning (see Chapter 21).20,22,23 The relative parameters are also termed control parameters. Scaling control parameters leads to a change in motor behavior to accomplish the task. For example, writing your name on the blackboard exemplifies scaling force, timing, and amplitude. Scaling is the proportional increase or decrease of the parameter to produce the intended motor activity.
Timing of muscle on/off activation for antagonistic muscles such as biceps and triceps, or hamstrings and quadriceps, needs to be accurate for coordination and control of movement patterns. If one muscle group demonstrates a delayed onset or maintains a longer duration of activity, overlapping with triceps “on” time, the movement will appear uncoordinated. Patients with neurological dysfunction often demonstrate alterations in the timing of muscle activity within functional synergies and in coupling functional synergies to produce movement.24,25 These functional movement synergies are not hardwired but represent emergent properties. They are flexible and adaptable to meet the challenges of the task and the environmental constraints.
Finite number of movement strategies
The concept of emergent properties could conceivably imply an unlimited number of movement strategies available to perform a particular task. However, limiting the degrees of freedom decreases the number of strategies available for selection. In addition, constraints imposed by the internal environment (e.g., musculoskeletal system, cardiovascular system, metabolic activity, cognition) and external environment (e.g., support surface, obstacles, lighting) limit the number of movement strategies. Horak and Nashner26 observed that a finite number of balance strategies were used by individuals in response to externally applied linear perturbations on a force plate system. With use of a life span approach, VanSant27 identified a limited number of movement patterns for the upper limb, head-trunk, and lower limb for the task of rising from supine to standing.
Variability of movements implies normalcy
Motivation to accomplish a task in spite of functional limitations and neuropathological conditions can also shift the individual’s CNS to select different patterns of motor behavior. The musculoskeletal system, by nature of the architecture of the joints and muscle attachments, can be a constraint on the movement pattern. An individual with a functional contracture may be limited in the ability to bend a joint only into a desired range, thereby decreasing the movement repertoire available to the individual. Such a constraint produces adaptive motor behavior. Dorsiflexion of the foot needs to meet a critical degree of toe clearance during gait. If there is a range of motion limitation in dorsiflexion, then biomechanical constraints imposed on the nervous system will produce adaptive motor behaviors (e.g., toe clearance during gait). Changes in motor patterns during the task of rising from supine to standing are observed when healthy individuals wear an orthosis to limit dorsiflexion.28 The inability to easily open and close the hand with rotation may lead to adaptations that require the shoulder musculature to place the hand in a more functional position. This adaptation uses axial and trunk muscles and will limit the use of that limb in both fine and gross motor performance. Refer to Chapter 23.
Preferred, nonobligatory movement patterns that are stable yet flexible enough to meet ever-changing environmental conditions are considered attractor states. Individuals can choose from a variety of movement patterns to accomplish a given task. For example, older adults may choose from a variety of fall-prevention movement patterns when faced with the risk of falling. The choice of motor plan may be negatively influenced by age-related declines in the sensory input systems or a fear of falling. For example, when performing the Multi-Directional Reach Test,29 an older adult may choose to reach forward, backward (lean), or laterally without shifting the center of gravity toward the limits of stability. This person has the capability of performing a different reaching pattern if asked, but prefers a more stable pattern.
Obligatory and stereotypical movement patterns also arise from external constraints imposed on the organism. Consider the external constraints placed on a concert violin player. These external constraints include, for example, the length of the bow and the position of the violin. Repetitive movement patterns leading to cumulative trauma disorder in healthy individuals can lead to muscular and neurological changes.30–33 Over time, changes in dystonic posturing and changes in the somatosensory cortex have been observed. Although one hypothesis considers that the focal dystonia results from sensory integrative problems, the observable result is a stereotypical motor problem.
Errors in motor control
Errors occur in the perception of sensory information, in selection of the appropriate MP, in selection of the appropriate variable parameters, or in the response execution. Patients with neurological deficits may demonstrate a combination of these errors. Therefore an assessment of motor deficits in clients includes analysis of these types of errors. If a therapist observes a motor control problem, there is no guarantee that the central problem arises from within the motor system. Somatosensory problems can drive motor dysfunction; cognitive and emotional problems express themselves through motor output. Thus it is up to the movement specialist to differentiate the cause of the problem through valid and reliable examination tools (see Chapter 8). Once the cause of the motor problem has been identified, selection of interventions should lead to more outcomes.
Motor control section summary
Motor control theories have been developed and have evolved over many years as our understanding of nervous system structure and function has become more advanced. The control of posture and movement is a complex process that involves many structures and levels within the human body. It requires accurate sensory inputs, coordinated motor outputs, and central integrative processes to produce skillful, goal-directed patterns of movement that achieve desired movement goals. We must integrate and filter multiple sensory inputs from both the internal environment of the body and the external world around us to determine position in space and choose the appropriate motor plan to accomplish a given task. We combine individual biomechanical and muscle segments of the body into complex movement synergies to deal with the infinite “degrees of freedom” available during the production of voluntary movement. Well learned motor plans are stored and retrieved and modified to allow for flexibility and variety of movement patterns and postures. When the PNS or CNS is damaged and the control of movement is impaired, new, modified, or substitute motor plans can be generated to accomplish goal-directed behaviors, remain adaptable to changing environments, and produce variable movement patterns. The process of learning new motor plans and refining existing behaviors by driving neuroplastic changes in the nervous system is discussed in the next sections of this chapter. The control of posture and balance is also discussed in Chapter 22.
Motor learning
Motor learning results in a permanent change in the performance of a skill because of experience or practice.34 The end result of motor learning is the acquisition of a new movement, or the reacquisition and/or modification of movement.35 The patient must be able to prepare and carry out a particular learned movement36 in a manner that is efficient (optimal movement with the least amount of time, energy, and effort),37 consistent (same movement over repeated trials),38 and transferrable (ability to perform movement under different environments and conditions) to be considered to have learned a skill.
Related posts:
 Differential diagnosis phase 1: medical screening by the therapist
Differential diagnosis phase 1: medical screening by the therapist
 Balance and vestibular dysfunction
Balance and vestibular dysfunction
