1
Clinical pelvic anatomy
Introduction
A thorough understanding of pelvic anatomy is essential for clinical practice. Not only does it facilitate an understanding of the process of labour, it also allows an appreciation of the mechanisms of sexual function and reproduction, and establishes a background to the understanding of gynaecological pathology. Congenital abnormalities are discussed in Chapter 5.
Obstetric anatomy
The bony pelvis
The girdle of bones formed by the sacrum and the two innominate bones has several important functions (Fig. 1.1). It supports the weight of the upper body, and transmits the stresses of weight bearing to the lower limbs via the acetabulae. It provides firm attachments for the supporting tissues of the pelvic floor, including the sphincters of the lower bowel and bladder, and it forms the bony margins of the birth canal, accommodating the passage of the fetus during labour.
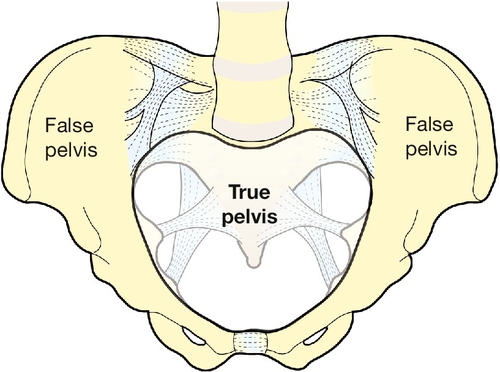
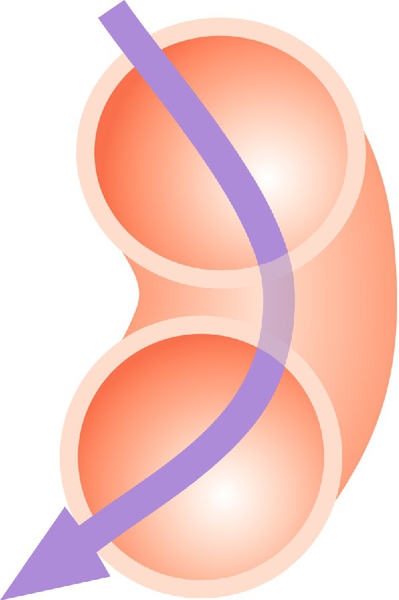
The birth canal is bounded by the true pelvis, i.e. that part of the bony girdle which lies below the pelvic brim – the lower parts of the two innominate bones and the sacrum. These bones are bound together at the sacroiliac joints, and at the symphysis pubis anteriorly. The brim is outlined by the promontory of the sacrum, the sacral alae, the iliopectineal lines and the symphysis. The pelvic outlet is bounded by bone and ligament including the tip of the sacrum, the sacrotuberous ligaments, the ischial tuberosities, and the subpubic arch (of rounded ‘Norman’ shape) formed by the fused rami of the ischial and pubic bones. In the erect posture the pelvic brim is inclined at an angle of 65–70° to the horizontal. Because of the curvature of the sacrum, the axis of the pelvis (the pathway of descent of the fetal head in labour) is a J-shaped curve (Fig. 40.4).
The change in the cross-sectional shape of the birth canal at different levels is fundamentally important in understanding the mechanics of labour. The canal can be envisaged initially as a sector of a curved cylinder of about 12 cm diameter (Fig. 1.2). The stresses of weight bearing at the brim level in the average woman tend to flatten the inlet a little, reducing the anteroposterior diameter, but increasing the transverse diameter. In the lower pelvis, the counterpressure through the necks of the femora tends to compress the pelvis from the sides, reducing the transverse diameters of this part of the pelvis (Figs 40.2 and 40.3). At an intermediate level, opposite the third segment of the sacrum, the canal retains a circular cross-section. With this picture in mind, the ‘average’ diameters of the pelvis at brim, cavity, and outlet levels can be readily understood (Table 1.1).
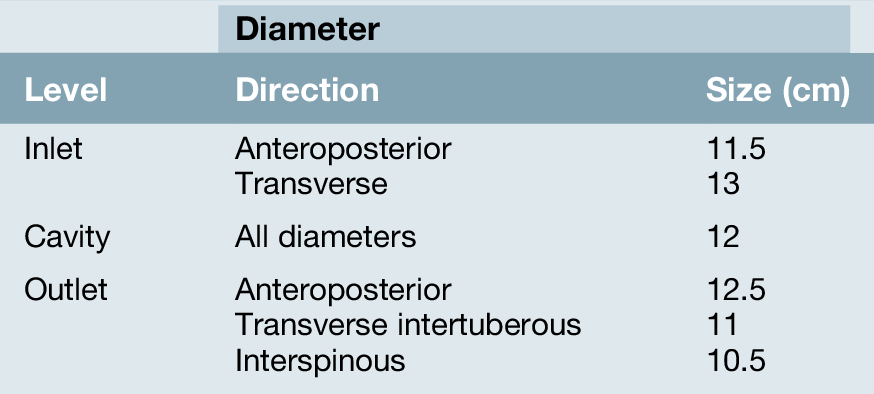
The distortions from a circular cross-section, however, are very modest. If, in circumstances of malnutrition or metabolic bone disease, the consolidation of bone is impaired, more gross distortion of the pelvic shape is liable to occur, and labour is likely to involve mechanical difficulty. This is termed cephalopelvic disproportion. The changing cross-sectional shape of the true pelvis at different levels – transverse oval at the brim and anteroposterior oval at the outlet – usually determines a fundamental feature of labour, i.e. that the ovoid fetal head enters the brim with its longer (anteroposterior) diameter in a transverse or oblique position, but rotates during descent to bring the longer head diameter into the longer anteroposterior diameter of the outlet before the time of birth. This rotation is necessary because of the relatively large size of the human fetal head at term, which reflects the unique size and development of the fetal brain (Fig. 45.1).
In most affluent countries, marked pelvic deformation is rare. Pelvimetry using X-rays, CT or MRI scans can be used to measure the pelvic diameters but is of limited clinical value in predicting the likelihood of a successful vaginal delivery. Mechanical difficulty in labour is assessed by close observation of the progress of dilatation of the cervix, and of descent, assessed by both abdominal and vaginal examination.
The pelvic organs during pregnancy
The uterus
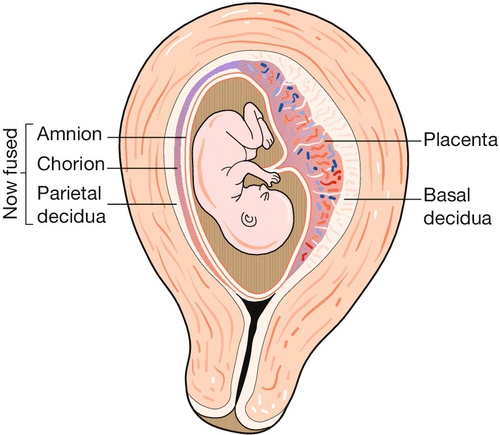
The uterus is a remarkable organ, composed largely of smooth muscle, the myometrium, which increases in weight during pregnancy from about 40 g to around 1000 g as the myometrial muscle fibres undergo both hyperplasia and hypertrophy (Fig. 1.3). It provides a ‘protected’ implantation site for the genetically ‘foreign’ fertilized ovum, accommodates the developing fetus as it grows, and finally expels it into the outside world during labour.
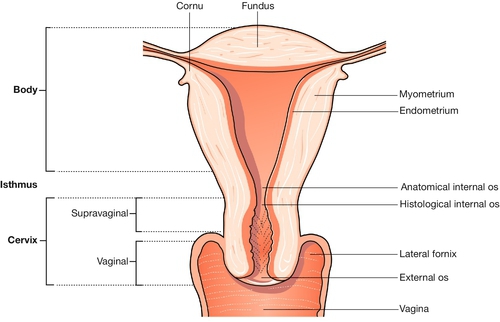
Whereas the body of the uterus is formed from a thick layer of plain muscle, the cervix, which communicates with the upper vagina, is largely composed of denser collagenous tissue. This forms a rigid collar, retaining the fetus in utero as the myometrium hypertrophies and stretches. The junctional area between the body and cervix is known as the isthmus, which, in late pregnancy and labour, undergoes dilatation and thinning, forming the lower segment of the uterus. It is through this thinned area that the uterine wall is incised during caesarean section.
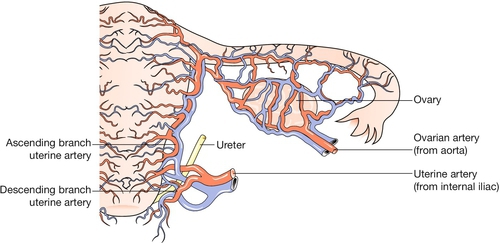
The uterine arteries, branches of the anterior division of the internal iliac arteries, become tortuous and coiled within the uterine wall (Fig. 1.4). Innervation of the uterus is derived from both sympathetic and parasympathetic systems, and the functional significance of the motor pathways is incompletely understood. Drugs which stimulate alpha-adrenergic receptors activate the myometrium, whereas beta-adrenergic drugs have an inhibitory effect, and both beta-agonists and alpha-antagonists have been used in attempts to inhibit premature labour. Afferent fibres from the cervix enter the cord via the pelvic splanchnic (parasympathetic) nerves (S2,3,4). Pain stimuli during labour from the fundus and body of the uterus travel via the hypogastric (sympathetic) plexus, and enter the cord at the level of the lower thoracic segments.
The cervix
This becomes more vascular and softens in early pregnancy. The mucous secretion from the endocervical glands becomes thick and tenacious, forming a mechanical barrier to ascending infection. In late pregnancy the cervix ‘ripens’ – the dense mesh of collagen fibres loosens, as fluid is taken up by the hydrophilic mucopolysaccharides which occupy the interstices between the collagen bundles. This allows the cervix to become shorter as its upper part expands.
Additional changes
The ligaments of the sacroiliac and symphyseal joints become more extensible under the influence of pregnancy hormones. As a result, the pelvic girdle has more ‘give’ during labour. The increased mobility of the joints may result in backache or symphyseal pain.
The urinary tract in pregnancy
Frequency of micturition is often noticed in early pregnancy. As pregnancy advances, the ureters become dilated, probably due to the relaxing effect of progesterone on the smooth muscle wall, but also in part due to the mechanical effects of the gravid uterus. The urinary tract is therefore more vulnerable to ascending infection (acute pyelonephritis) in comparison to non-pregnancy.
The perineum
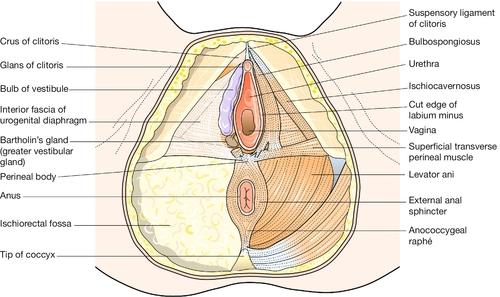
This term usually refers to the area of skin between the vaginal orifice and the anus. The underlying musculature at the outlet of the pelvis, surrounding the lower vagina and the anal canal, is important in the maintenance of bowel and urinary continence, and in sexual response. The muscles intermesh to form a firm pyramidal support, the perineal body, between the lower third of the posterior vaginal wall and the anal canal (Fig. 1.5). The tissues of the perineal body are often markedly stretched during the expulsive second stage of labour and may be torn as the head is delivered. Injury to the anal sphincters may lead to impaired anal continence of faeces and/or flatus. Poor healing of an episiotomy or tear is liable to result in scarring, which may cause dyspareunia (pain during intercourse).
Anatomical points for obstetric analgesia
Pudendal nerve block
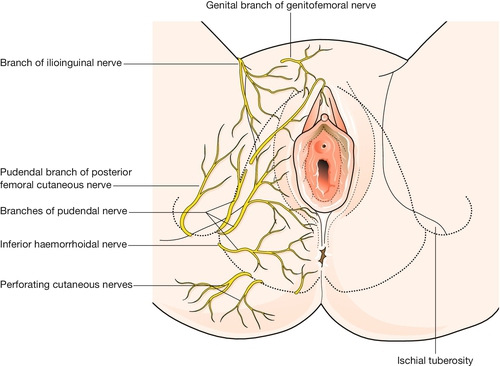
Knowledge of the pudendal nerves is important in obstetrics because they may be blocked to minimize pain during instrumental delivery, and because their integrity is vital for visceral muscular support and for sphincter function. These nerves, which innervate the vulva and perineum, are derived from the second, third and fourth sacral roots (Fig. 1.2). On each side the nerve passes behind the sacrospinous ligament close to the tip of the ischial spine, and re-enters the pelvis along with the pudendal blood vessels in the pudendal canal. After giving off an inferior rectal branch, they divide into the perineal nerves and the dorsal nerves of the clitoris. Motor fibres of the pudendal nerve supply the levator ani, the superficial and deep perineal muscles, and the voluntary urethral sphincter. Sensory fibres innervate the central areas of the vulva and perineum. The peripheral skin areas are supplied by branches of the ilioinguinal nerve, the genitofemoral nerve, and the posterior femoral cutaneous nerve (Fig. 1.6). The pudendal nerve can be blocked by an injection of local anaesthetic just below the tip of the ischial spine, as described on page 346.
Spinal block
The spinal cord ends at the level of L1–2. A spinal injection at the level of the L3–4 space will produce excellent analgesia up to around the level of the T10 nerve root or above, depending on the position of the patient and the volume of local anaesthetic used.
Epidural block
The epidural space, between the dura and the periosteum and ligaments of the spinal canal, is about 4 mm deep. Epidural injection of local anaesthetic blocks the spinal nerve roots as they traverse the space.
Gynaecological anatomy
The uterus
The uterus has the shape of a slightly flattened pear, and measures 7.5 × 5.0 × 2.5 cm. Its principal named parts are the fundus, the cornua, the body and the cervix (Fig. 1.7).
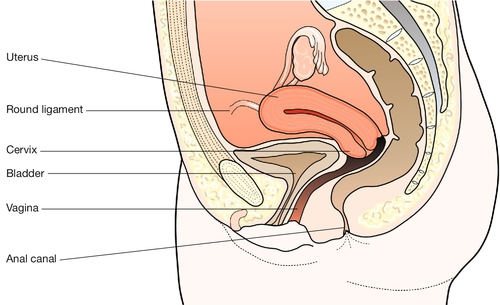
It forms part of the genital tract, lying in close proximity to the urinary tract anteriorly, and the lower bowel behind. All three tracts traverse the pelvic floor in the hiatus between the two bellies of the levator ani muscle. Clinically this means that a problem in one tract can readily affect another (Fig. 1.8).
The uterine cavity is around 6 or 7 cm in length, and forms a flattened slit, with the anterior and posterior walls in virtual contact. The wall has three layers: the endometrium (innermost), the myometrium and the peritoneum (outermost).




