± dilation of upstream intrahepatic ducts, as associated periductal fibrosis may impede ductal dilatation
• Distribution of strictures in biliary tree reflects hepatic arterial supply to bile ducts
Proximal extrahepatic duct and biliary confluence strictures are most common due to blood supply from hepatic artery
Distal extrahepatic duct is supplied by gastroduodenal artery branches, and consequently usually not involved
Gallbladder and cystic duct may be involved
Rarely causes peripheral intrahepatic strictures
• CT or MR: Involved bile ducts may show periductal edema, mural thickening, and enhancement
• Biloma formation (± abscess formation) may reflect drug-induced necrosis of peripheral ducts
TOP DIFFERENTIAL DIAGNOSES
• Primary sclerosing cholangitis
• Autoimmune cholangitis
• Extrinsic compression by liver masses or lymphadenopathy
• Chemical or drug-induced liver injury
PATHOLOGY
• Results from either direct toxic effects of drug on biliary ducts or fibrosis/occlusion of peribiliary vascular plexus with resultant biliary ischemic cholangiopathy
• Risk factors: Preexisting biliary strictures, prior biliary surgery, portal vein occlusion, nonselective placement of catheter during chemoembolization, higher doses of chemotherapy
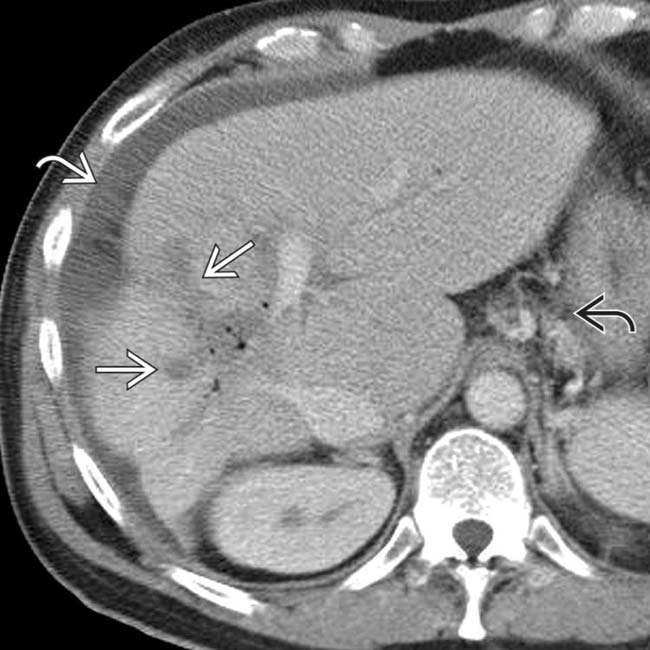
(Left) Axial CECT shows a liver metastasis that is low in attenuation, likely as a result of necrosis. Note the dilated ducts that resulted from a stricture of the biliary bifurcation and common hepatic duct, also due to chemotherapy.
(Right) Transhepatic cholangiogram in the same patient shows gross dilation of the intrahepatic ducts, with abrupt, high-grade stenosis at the confluence of the right and left ducts. This patient had received floxuridine through an arterial catheter .
(Left) CECT of a patient with carcinoid liver metastases after 8 courses of TACE shows irregular right periductal low attenuation , pneumobilia, posterior segment atrophy, gastroesophageal varices , and ascites , compatible with chemotherapy-induced cholangitis and biliary cirrhosis.
(Right) ERCP of the same patient shows a proximal common duct stricture and irregular, strictured intrahepatic ducts. A liver transplant was performed with cholangitis, bilomas, and biliary cirrhosis identified within the explant.
• Iatrogenic cholangitis following intraarterial chemotherapy for hepatic malignancies or metastases
Complication of hepatic artery infusion pump (HAIP) or transarterial chemoembolization (TACE)
IMAGING
General Features
• Location
Distribution of strictures in biliary tree reflects hepatic arterial supply to bile ducts
– Proximal extrahepatic duct and central intrahepatic ducts/biliary confluence are most commonly involved (∼ 50%) due to blood supply from hepatic artery branches
– Distal extrahepatic duct supplied by gastroduodenal artery branches, and consequently not usually involved
 Proximal extrahepatic duct and biliary confluence strictures are most common due to blood supply from hepatic artery
Proximal extrahepatic duct and biliary confluence strictures are most common due to blood supply from hepatic artery




 that is low in attenuation, likely as a result of necrosis. Note the dilated ducts
that is low in attenuation, likely as a result of necrosis. Note the dilated ducts  that resulted from a stricture of the biliary bifurcation and common hepatic duct, also due to chemotherapy.
that resulted from a stricture of the biliary bifurcation and common hepatic duct, also due to chemotherapy.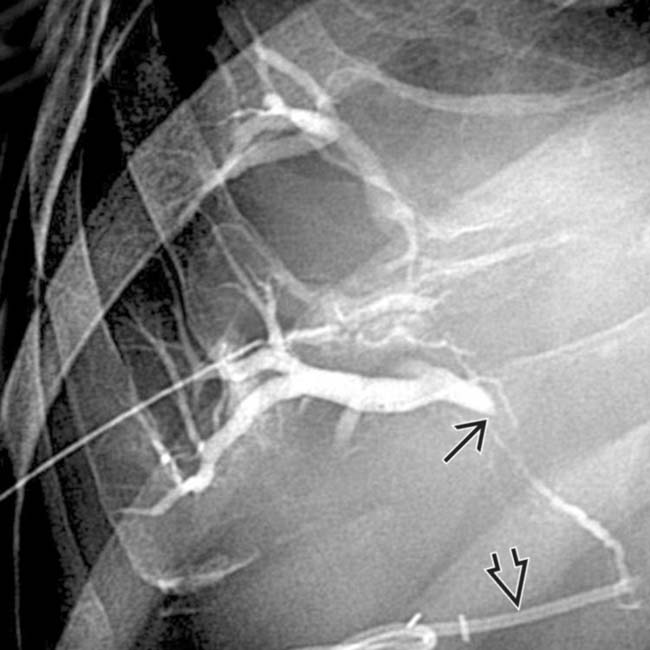
 at the confluence of the right and left ducts. This patient had received floxuridine through an arterial catheter
at the confluence of the right and left ducts. This patient had received floxuridine through an arterial catheter  .
.
 , pneumobilia, posterior segment atrophy, gastroesophageal varices
, pneumobilia, posterior segment atrophy, gastroesophageal varices  , and ascites
, and ascites  , compatible with chemotherapy-induced cholangitis and biliary cirrhosis.
, compatible with chemotherapy-induced cholangitis and biliary cirrhosis.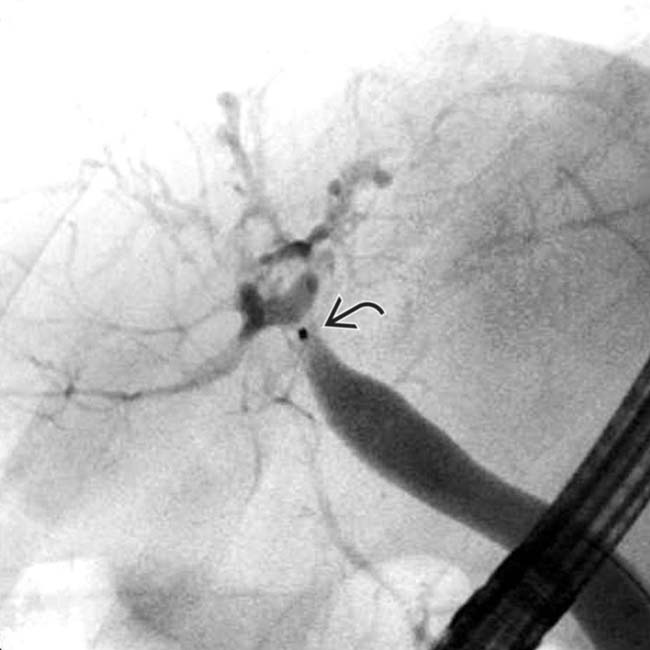
 and irregular, strictured intrahepatic ducts. A liver transplant was performed with cholangitis, bilomas, and biliary cirrhosis identified within the explant.
and irregular, strictured intrahepatic ducts. A liver transplant was performed with cholangitis, bilomas, and biliary cirrhosis identified within the explant.
 Distribution of strictures in biliary tree reflects hepatic arterial supply to bile ducts
Distribution of strictures in biliary tree reflects hepatic arterial supply to bile ducts





