CHAPTER 12 Capsulorrhexis and hydrodissection

Capsulorrhexis
Background
Continuous curvilinear capsulorrhexis (CCC) is the most reliable way of creating a secure and resilient opening in the lens capsule and was originally developed for use in phacoemulsification surgery where it has now been universally adopted1,2. It has more recently gained widespread popularity in the developing world for use in manual small incision cataract surgery (MSICS)3. The ‘three Cs’ also conveniently represent the three principal technical challenges, which require the rhexis to be Circular, Central, and the Correct size.
Instruments
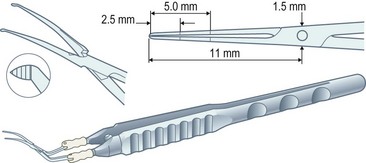
Capsulorrhexis forceps, on the other hand, allow you to apply traction in any chosen direction but are relatively bulky (particularly the early parallel-action Utratta designs) and are more likely to cause wound gape and chamber collapse than a needle. However the newer designs are greatly refined and include hinged ‘cross-action’ and coaxial designs that cause minimal wound gape and give exquisite control of the tear through incisions down to sub-2 mm (Fig. 12.1). The high outlay cost, difficulty in cleaning, and susceptibility to damage of capsulorrhexis forceps all ensure that the bent needle is here to stay.
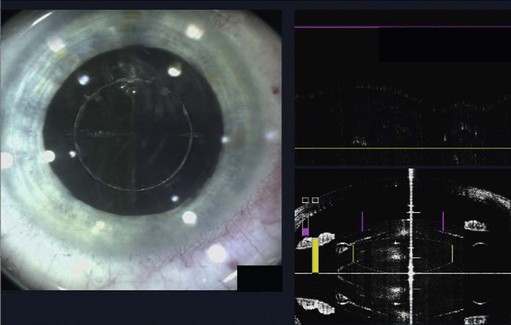
The role of lasers in surgery is assuming an ever-increasing importance and, at the time of writing, the femtosecond laser has recently been used successfully on human eyes to create high precision incisions and accurate capsulorrhexis (Fig. 12.2).