CHAPTER 26 Arthroscopic Treatment of Triangular Fibrocartilage Complex Injuries
The triangular fibrocartilage complex (TFCC) is a complex anatomical structure located at the ulnar side of the wrist. It has the important biomechanical function of providing stability to both the ulnar carpus and the distal radioulnar joint (DRUJ). Disorders of the TFCC are responsible for the ulnar-sided wrist symptoms of pain, weakness, and instability that affect function. The diagnosis and treatment of these injuries to the TFCC will restore stability, resulting in pain relief and a good prognosis for return of function.
Anatomy
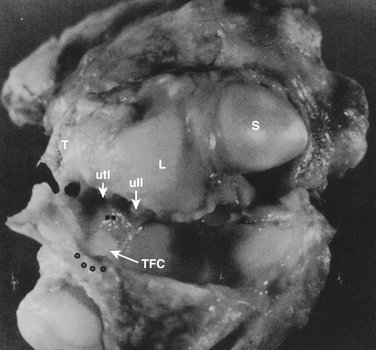
The TFCC is a cartilaginous and ligamentous structure interposed between the ulnar carpus and the distal ulna (Fig. 26-1). It arises from the distal aspect of the sigmoid notch of the radius and inserts into the base of the ulnar styloid. The TFCC attaches to the ulnar carpus via the ulnocarpal ligament complex (ulnolunate, ulnotriquetral, and ulnar collateral ligaments).1–3 The radioulnar ligaments stabilize the DRUJ, limiting rotational as well as axial migration.4 The dorsal and volar radioulnar ligaments (Fig. 26-2) are fibrous thickenings within the substance of the TFCC. As a result of this anatomical configuration, they function as a unit rather than as independent ligaments. The central, horizontal portion of the TFCC is the thinnest portion, composed of interwoven obliquely oriented sheets of collagen fibers5 for the resistance of multidirectional stress.
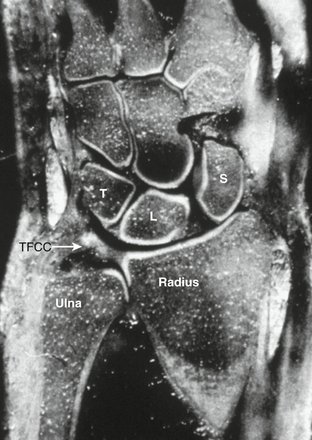
FIGURE 26-1 Anatomical coronal section demonstrating the TFCC and relation to the lunate (L), triquetrum (T), scaphoid (S), and distal ulna and radius.
(From Palmer AK, Werner FW: The triangular fibrocartilage complex of the wrist—anatomy and function. J Hand Surg. 1981; 6A:154.)
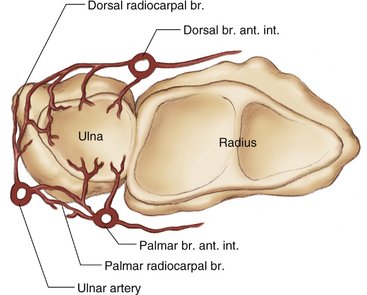
The vascularity of the TFCC has been carefully studied.5–7 The TFCC receives its blood supply from the ulnar artery through its radiocarpal branches and the dorsal and palmar branches of the anterior interosseous artery (Fig. 26-3). These vessels supply the TFCC in a radial fashion. Histologic sections demonstrate that these vessels penetrate only the peripheral 10% to 40% of the TFCC. The central section and radial attachment is avascular (Fig. 26-4). This vascular anatomy supports the concept that peripheral injuries possess the ability to heal if injured and treated appropriately, whereas the tears of the central portion do not heal if sutured and are usually débrided.

Biomechanics
The TFCC has several important biomechanical functions. It transmits 20% of an axially applied load from the ulnar carpus to the distal ulna, it is the major stabilizer of the DRUJ, and it is a stabilizer of the ulnar carpus.3,8–12
The amount of the load transferred to the distal ulna varies with ulnar variance. A greater amount is transferred in ulnar-positive variance than ulnar-negative variance. This results in a corresponding decreased thickness of the central portion of the TFCC in ulnar-positive wrists.10 In addition, there is a variable load placed on the TFCC with forearm rotation. Supination causes ulnar-negative variance owing to the proximal migration of the ulna. This is reversed with pronation as the ulna moves distally, causing it to become ulnar positive.13 The ulnar head also moves within the sigmoid notch in a dorsal direction with pronation and volar with supination.8 The dorsal and volar radioulnar ligaments that form the peripheral portion of the TFCC become tight with forearm rotation, serving as major stabilizers of the DRUJ, which control this translation during rotation.9
Mechanism of Injury
Traumatic injuries of the TFCC result from the application of an extension/pronation force to the axially loaded wrist or by a distraction force to the ulnar aspect of the wrist.1,14 This will most commonly occur with a fall on the outstretched hand. The lesions are more common with ulnar-positive and ulnar-neutral patients and are commonly found in those patients being treated for fractures of the distal radius.
Several authors have examined the incidence of intracarpal soft tissue injuries associated with distal radial fractures. Geissler and coworkers15 studied 60 patients, finding a TFCC injury in 26 (43%). In Lindau and colleagues’ series of 51 patients,16 a TFCC injury was found in 43 (84%): 24 had a peripheral tear, 10 had a central perforation, and 9 had a combined central and peripheral tear. Richards and associates in their series of 118 patients17 reported a TFCC injury in 35% of the patients with intra-articular fractures and 53% of those with extra-articular fractures.
Classification
The classification system described by Palmer1 is the most useful for describing TFCC injuries that are both traumatic and degenerative. Only traumatic lesions are discussed here.
A class 1A lesion represents a tear in the horizontal or central portion of the TFCC (Fig. 26-5A). The tear is 2 to 3 mm medial to the radial attachment of the cartilage. It is usually oriented from dorsal to volar.
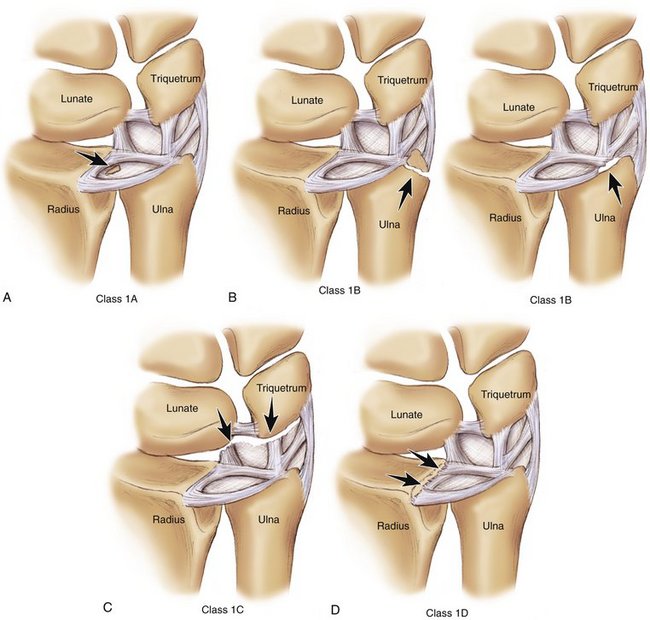
A class 1B lesion (see Fig. 26-5B) is an avulsion of the peripheral aspect of the TFCC from its insertion onto the distal ulna. This can occur either with a fracture of the ulnar styloid or as a pure avulsion from its bony attachment. This type of injury disrupts the stabilizing effect of the TFCC on the DRUJ, resulting in clinical instability.
A class 1C lesion (see Fig. 26-5C) is an avulsion of the TFCC attachment to the ulnar carpus by disruption of the ulnocarpal ligaments. This lesion will result in ulnar carpal instability with volar translocation of the carpus.
A class 1D lesion (see Fig. 26-5D) is an avulsion of the TFCC from its radial attachment. Involvement of the dorsal and or volar radioulnar ligaments will result in instability of the DRUJ.
Diagnosis
Clinical symptoms consist of ulnar-sided wrist pain frequently with clicking and typically occur after a fall. The initial physical examination reveals swelling over the ulnar aspect of the wrist with inflammation of the tendon of the extensor carpi ulnaris. Point tenderness is present over the TFCC and distal ulna. Ulnar deviation and axial loading of the wrist (TFCC compression test) (Fig. 26-6) will elicit a painful response. A click is frequently present with forearm rotation. The DRUJ must be assessed for instability. Instability is best assessed with the forearm in neutral rotation, but it is also checked in full supination and full pronation. The examiner stabilizes the distal radius with one hand and applies a force to the distal ulna, moving it dorsal and volar in a search for increased motion or subluxation of the distal ulna relative to the radius compared with the opposite uninjured wrist. Significant instability would present as laxity of the distal ulna with a positive “piano key“ sign and dorsal prominence of the distal ulna. This would represent a significant tear or detachment of the dorsal or volar radioulnar ligaments.

FIGURE 26-6 TFCC compression test: ulnar deviation and axial load applied to wrist produces a painful response.
TFCC injuries do not occur in isolation but are a component of a spectrum of injury to the ulnar side of the wrist.18 The examiner must therefore evaluate all of the commonly injured structures on the ulnar side of the wrist. The lunatotriquetral joint must be assessed for instability due to a lunatotriquetral ligament tear. This would cause tenderness over the lunatotriquetral interval with a positive shuck test. The dorsal radial carpal ligament complex should be examined to determine if traumatic midcarpal instability is present.
Imaging
Magnetic resonance imaging (MRI) is useful in the diagnosis of TFCC tears, especially the class 1A and D lesions.19,20 T2-weighted MR images in the coronal plane are of the greatest diagnostic value (Fig. 26-7). The TFCC has a homogeneous low signal intensity. The synovial fluid of the joint appears as a bright image on T2-weighted images and will outline tears in the TFCC. The addition of a gadolinium arthrogram enhances the visualization of TFCC tears.

The series in the literature reviewing the sensitivity and specificity of MRI in diagnosing injuries of the TFCC show significant variation in the reported results. Golimbu and coworkers19






