Chapter 150 Ankylosing Spondylitis and Other Spondyloarthritides
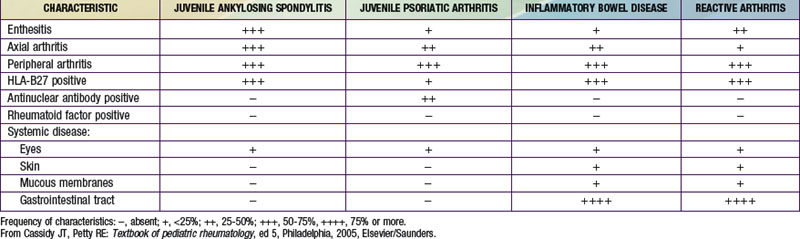
The diseases collectively referred to as spondyloarthritides include ankylosing spondylitis (AS), arthritis associated with inflammatory bowel disease (IBD) and psoriasis, and reactive arthritis following gastrointestinal or genitourinary infections (see Table 150-1 on the Nelson Textbook of Pediatrics website at www.expertconsult.com). Pediatric rheumatologists have adopted the International League of Associations for Rheumatology (ILAR) classification scheme for juvenile idiopathic arthritis (JIA) and use the term enthesitis-related arthritis (ERA) to encompass most forms of spondyloarthritis in children, except those with co-existing psoriasis.
at www.expertconsult.com). Pediatric rheumatologists have adopted the International League of Associations for Rheumatology (ILAR) classification scheme for juvenile idiopathic arthritis (JIA) and use the term enthesitis-related arthritis (ERA) to encompass most forms of spondyloarthritis in children, except those with co-existing psoriasis.
Etiology and Pathogenesis
Spondyloarthritides are complex genetic diseases in which susceptibility is largely genetically determined. HLA-B27 is responsible for around 40% of AS susceptibility, with genes encoding the interleukin-23 (IL-23) receptor (IL23R), ERAP1 (endoplasmic reticulum aminopeptidase-1; also known as ARTS-1 [type 1 tumor necrosis factor receptor shedding aminopeptidase regulator]), IL-1α (IL1A), and others playing important roles. Enteric infection with certain gastrointestinal or genital pathogens can trigger reactive arthritis (Chapter 151); environmental triggers for other forms of spondyloarthritis have not been identified. Although molecular mimicry between HLA-B27 and antigens from bacteria has been postulated as an underlying mechanism of disease, evidence supporting this hypothesis is scarce. Other unusual properties of HLA-B27, such as its tendency to misfold and form unusual cell surface structures, may play a role.
Clinical Manifestations
Enthesitis-Related Arthritis
Children are classified as having ERA if they have either arthritis and enthesitis or arthritis or enthesitis, with two of the following additional characteristics: (1) sacroiliac joint tenderness or inflammatory lumbosacral pain (see Table 150-1), (2) the presence of HLA-B27, (3) age > 6 yr and male sex, (4) acute anterior uveitis, and (5) a family history of an HLA-B27–associated disease (ERA, sacroiliitis with IBD, reactive arthritis, or acute anterior uveitis) in a first-degree relative. Patients with psoriasis (or a family history of psoriasis in a first-degree relative), a positive rheumatoid factor (RF) test result, or systemic arthritis are excluded from this group. Many children with ERA go on to eventually have AS, but many do not, and it is not currently possible to determine whose ERA will progress.
Juvenile Ankylosing Spondylitis
JAS frequently begins with oligoarthritis and enthesitis. The arthritis occurs predominantly in the lower extremities and often involves the hips, in contrast to oligoarticular JIA. Also unlike in adult-onset AS, in JAS axial involvement is usually absent until later in the disease course (Fig. 150-1). Enthesitis is particularly common, manifesting as localized and often severe tenderness at characteristic tendon (as well as ligament, fascia or capsule) insertions around the plantar surface of the foot, ankle (Achilles), and knee (patella). The disease course is variable and can include periods of low disease activity. Fever and weight loss are uncommon and, if present, raise the possibility of IBD.



