CHAPTER 76
Posterior Cruciate Ligament Sprain
Farshad Adib, MD; Christine Curtis, MD; Peter Bienkowski, MD; Lyle J. Micheli, MD
Definition
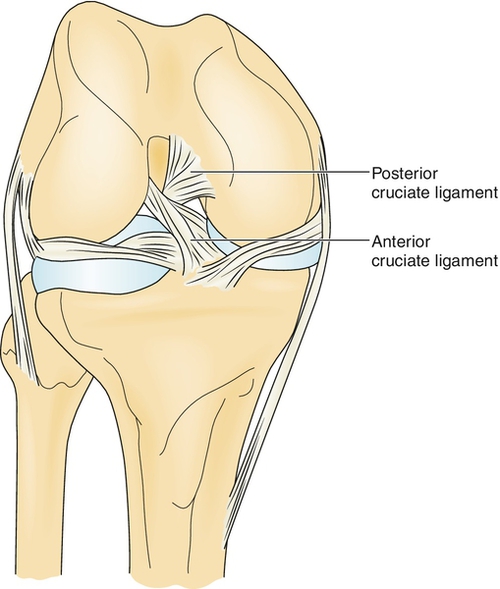
Posterior cruciate ligament (PCL) tears represent 5% to 38% of all knee ligament injuries [1,2]. The PCL is an intra-articular but extrasynovial structure that arises from the posterior aspect of the tibial plateau (about 1 cm distal to the joint line), crosses (“cruciate”) behind the anterior cruciate ligament (ACL), and inserts into the lateral portion of the medial femoral condyle (Fig. 76.1). The main function of the PCL is to resist posterior displacement of the tibia on the femur. It also acts as a secondary restraint to external tibial rotation. The PCL also has some restraint against varus and valgus forces. The larger and stronger anterolateral bundle is tight in flexion, whereas the posteromedial bundle is tight in extension. The anterior meniscofemoral ligament (Humphry) and posterior meniscofemoral ligament (Wrisberg) make a Y-shaped sling around the PCL [3]. The average distance between the center of the femoral attachments of anterolateral and posteromedial bundles is 12.1 ± 1.3 mm; this distance on the tibial side is 8.9 ± 1.2 mm [4].
Together with the ACL, the PCL functions in the “screw-home” mechanism of the knee by which the tibia glides to its exact position at terminal knee extension. In general, PCL tears occur in a flexed knee when the tibia is displaced posteriorly. This can occur in a motor vehicle accident (dashboard injury) or during a fall on a flexed knee with the foot in plantar flexion. The PCL may also rupture from hyperextension and rotation on a planted foot or on forced hyperflexion. PCL injuries may occur in isolation, but they generally occur with other injuries (e.g., ACL tear, collateral ligament tear, and meniscal injuries).
In a chronic PCL-deficient knee, an increase of force on the medial and patellofemoral compartments might lead to development of early degenerative arthritis [5]. In contrast to ACL injuries, most series of PCL injuries have reported a higher incidence of injury to men [6]. Fewer studies have been done about PCL injuries in comparison to ACL injuries.
Symptoms
It is important to obtain information about the nature of the injury. Typically, patients report that they have fallen on a flexed knee or have sustained a blow to the anterior knee when it was flexed (e.g., on the dashboard of a car). Rarely, patients may recall feeling or hearing a “pop” at the time of injury (more common in ACL tear). Patients may have pain in the posterior aspect of the knee in the acute cases or along the medial or patellofemoral region in the chronic cases.
Patients may report instability, stiffness, and an inability to bear weight and to walk. Swelling can range from insignificant to very swollen.
Physical Examination
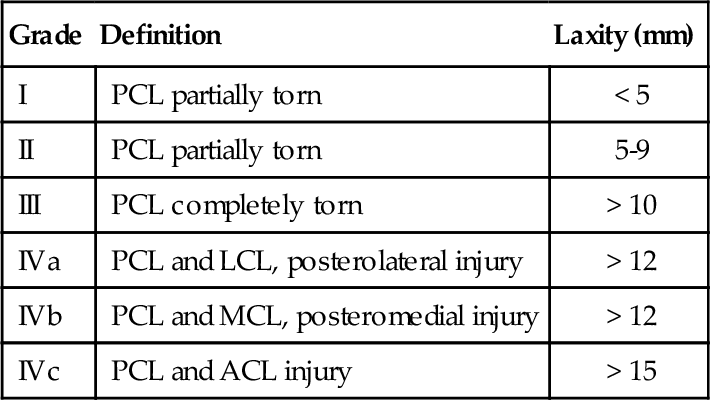
In an acute injury, there may be contusion of the anterior tibia, and popliteal ecchymosis may be present. Swelling and effusion will vary and may not be present at all. Limb alignment, gait pattern, and range of motion should be evaluated. See Table 76.1 for the general classifications of PCL injuries. It has been shown that a grade III on posterior drawer testing and posterior tibial translation on stress radiography of more than 10 mm correlate with the presence of a posterolateral corner injury in addition to a complete disruption of the PCL [7].
It is essential during the examination of the knee to evaluate all knee ligaments thoroughly to identify combined ligamentous injuries. The goal of PCL evaluation is to identify posterior subluxation of the tibia, which occurs with PCL insufficiency.
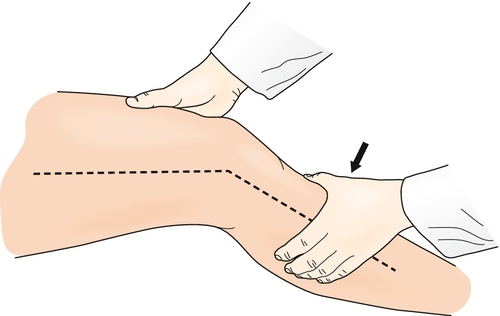
The “gold standard” of PCL examination is the posterior drawer test (Fig. 76.2). During this test, the knee is flexed at 90 degrees with the hip held at 45 degrees of flexion. It is essential to appreciate a normal 1-cm step-off of the medial tibial plateau anterior to the medial femoral condyle. The absence of the step-off should alert the clinician to a possibility of PCL injury. Posterior pressure is applied to the tibia while the amount of displacement of the medial tibial step-off and the quality of the endpoint in comparison with the contralateral knee are noted. Posterolateral instability may be evaluated by the posterior drawer test with the foot externally rotated 15 degrees. Similarly, posteromedial instability is assessed by the posterior drawer test with the foot internally rotated 15 degrees.

The posterior Lachman test involves positioning of the knee at 30 degrees of flexion with posterior pressure applied to the proximal tibia (Fig. 76.3). The extent of displacement and the quality of the endpoint are evaluated and compared with the contralateral knee.