CHAPTER 43
Thoracic Radiculopathy
Darren Rosenberg, DO; Daniel C. Pimentel, MD
Definition
Thoracic radiculopathy is a painful syndrome caused by mechanical compression, chemical irritation, or metabolic abnormalities of the thoracic spinal nerve root. Thoracic disc herniation accounts for less than 5% of all disc protrusions [1,2]. It accounts for less than 2% of all spinal disc surgeries and 0.15% to 4% of all symptomatic spinal disc herniations [3]. The majority of thoracic disc herniations (35%) occur between the levels of T8 and T12, with a peak (20%) at T11-12. Most patients (90%) present clinically between the fourth and seventh decades of life; 33% present between the ages of 40 and 49 years. Approximately 33% of thoracic disc protrusions are lateral, preferentially encroaching on the spinal nerve root. The remainder are central or central lateral, resulting primarily in various degrees of spinal cord compression. Synovial cysts, although rare in the thoracic spine (0.06% of patients requiring decompressive surgery), may also be responsible for foraminal encroachment. These tend to be more common at the lower thoracic levels [4].
Natural degenerative forces and trauma are generally thought to be the most important factors in the etiology of mechanical thoracic radiculopathy. Foraminal stenosis from bone encroachment may also cause compression of the exiting nerve root and radicular symptoms. Perhaps one of the most common metabolic causes of thoracic radiculopathy is diabetes, often resulting in multilevel disease [4]. This may occur at any age but often appears with other neuropathic symptoms due to injury to the blood supply to the nerve root. Finally, another etiology that should be considered a possible cause of thoracic radiculopathy is neoplastic compression. Primary spine tumors are rare, although the spine is a frequent metastasis site (4%-15%) of primary solid tumors, such as breast, lung, and prostate cancer [5]. Regarding spine metastasis, the thoracic spine is the most commonly affected (70%), followed by lumbar (20%) and cervical (10%) [6].
Symptoms
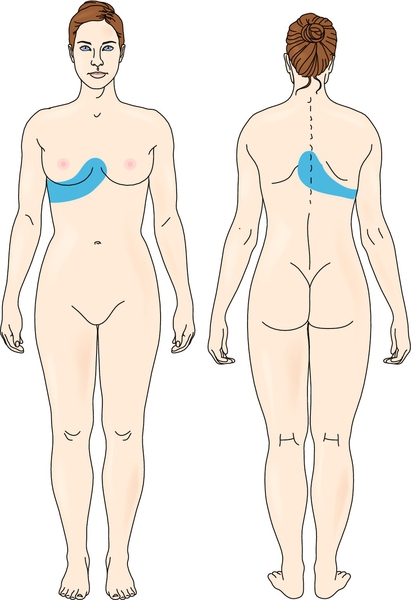
Most patients (67%) present with complaints of “band-like” chest pain (Fig. 43.1). The second most common symptom (16%) is lower extremity pain [7]. Injury to nerve roots T2-3 may be manifested as axillary or midscapular pain. Injury to nerve roots T7-12 may be manifested as abdominal pain [8]. Unlike thoracic radiculopathy, spinal cord compression produces upper motor neuron signs and symptoms consistent with myelopathy. Therefore examiners should pay close attention to the presence of motor impairment, hyperreflexia and spasticity, sensory impairment, and bowel and bladder dysfunction. The last may be caused by T11-12 lesions damaging the conus medullaris or cauda equina [9].
Thus, in thoracic radiculopathy, pain—localized, axial, or radicular—is the primary complaint in 76% of patients. It is also important to include in the history any trauma (present in 37% of patients) [10] or risk factors for non-neurologic causes of chest wall or abdominal pain. Thoracic compression fractures that may mimic the symptoms of thoracic radiculopathy may be seen in young people with acute trauma, particularly falls, regardless of whether they land on their feet. In older people (particularly women with a history of osteopenia or osteoporosis) or in individuals who have prolonged history of steroid use, a compression fracture should be considered. Because thoracic radiculopathy is not common, it is important in nontraumatic cases to be suspicious of more serious pathologic processes, such as malignant disease. Therefore a history of weight loss, decreased appetite, and previous malignant disease should be elicited.
Physical Examination
The physical examination may show only limitations of range of motion—particularly trunk rotation, flexion, and extension—generally due to pain. In traumatic cases, location of ecchymosis or abrasions should be noted. Range of motion testing should not be done repeatedly if an acute spinal fracture is suspected. Careful palpation for tenderness over the thoracic spinous and transverse processes as well as over the ribs and intercostal spaces is critical in localizing the involved level. Pain with percussion over the vertebral bodies should alert the clinician to the possibility of a vertebral fracture.
On the other hand, uncommon symptoms in the lower limbs, such as pain, reflex changes, spasticity, and weakness, can be a result of spinal cord compression by thoracic disc herniation [11], although this phenomenon is seldom observed.
Physical examination in diagnosis of thoracic radiculopathy has a modest accuracy and reliability because there is difficulty in testing strength of possibly affected muscles (such as paraspinal, intercostal, and abdominal muscles) isolatedly [12], although it is crucial for ruling out other possible causes of pain or neurologic abnormalities. In addition, sensation may be abnormal in a dermatomal pattern. This will direct the examiner to more closely evaluate the involved level. Any abnormalities of the spine should be noted, including scoliosis, which is best detected when the patient flexes forward. A thorough examination of the cardiopulmonary system, abdominal organs, and skin should be performed, particularly in individuals who have sustained trauma or relevant comorbidities.






