CHAPTER 31
Flexor Tendon Injuries
Definition
The flexor tendons of the hand are vulnerable to laceration and rupture. These injuries are most commonly seen in individuals who work around moving equipment, use knives, or wash glass dishes; in people with rheumatoid arthritis; and in athletes (jersey finger) [1]. The flexor digitorum profundus (FDP) of the ring finger is the most commonly involved [2]. Incomplete injuries to the flexor tendon are easily missed on physical examination and can progress to full ruptures.
Regions of potential tendon injury are divided into five zones (Fig. 31.1) [3]. Zone I is from the tendon insertion at the base of the distal phalanx to the midportion of the middle phalanx. Laceration or injury in this zone results in disruption of the FDP tendon and the inability to flex the distal interphalangeal (DIP) joint. Zone II extends from the midportion of the middle phalanx to the distal palmar crease. This zone is known as no man’s land because of the poor functional results after tendon repair [4,5]. Tendon injury in this zone usually involves both FDP and flexor digitorum superficialis (FDS) tendons and results in inability to flex the DIP and proximal interphalangeal (PIP) joints. Zone III is located from the distal palmar crease to the distal portion of the transverse carpal ligament. This zone includes the intrinsic hand muscles and vascular arches. Zone IV overlies the transverse carpal ligament in the area of the carpal tunnel. In this zone, injuries usually involve multiple FDP and FDS tendons. Zone V extends from the wrist crease to the level of the musculotendinous junction of the flexor tendons. Injuries in this region most often result from self-inflicted laceration (suicide attempts).
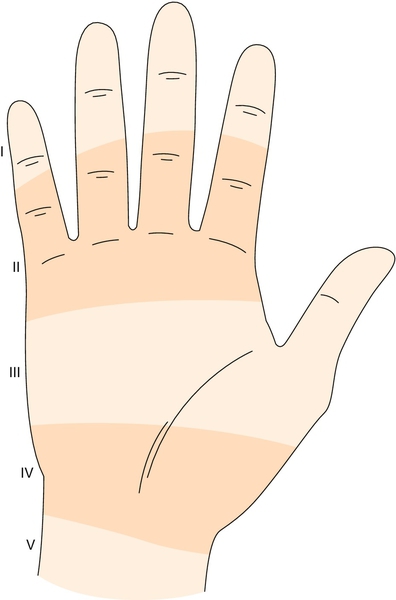
The flexor tendons are held close to the bone in zone I and zone II by a complex series of pulleys and vincula. These structures are frequently injured with the tendons [1].
Symptoms
On occasion, individuals may hear a popping sensation as the flexor tendon tears. This is followed by pain, swelling, and inability to flex the affected joint. Sensation of the involved finger is often affected because of the proximity of the flexor tendons to the neurovascular bundle.
Physical Examination
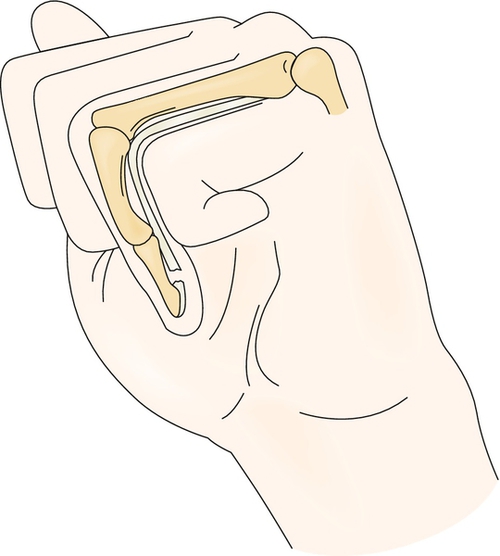
Obtaining a detailed history is important to outline the mechanism of injury. Evaluation begins with observation of the resting hand position. If the flexor tendon is completely severed, the unsupported finger will assume an extended position (Fig. 31.2) [1,6]. Active flexion of all finger joints needs to be assessed. If active finger flexion is not observed because of pain, tenodesis can be employed to determine whether the tendon is intact. The wrist is passively extended, and all fingers should assume a relatively flexed posture. If the flexor tendons are disrupted, the finger will remain in a relatively extended posture.
Flexion strength of each digit should be evaluated by manual muscle testing or finger dynamometry. Strength is evaluated by having the patient individually flex first the DIP joint and then the PIP joint against applied resistance. It is possible to have a complete laceration of the flexor tendons with preservation of peritendinous structures and active motion. In these cases, however, flexion will be weak [7].
For individual function of the FDP tendon to be checked, the patient is asked to flex the fingertip at the DIP joint while the PIP joint is maintained in extension. If there is injury to the FDP tendon, the patient will be unable to flex the DIP joint.






