CHAPTER 16
Rotator Cuff Tendinopathy
Definition
Rotator cuff tendinopathy is a common phenomenon affecting both athletes and nonathletes. The muscles that compose the rotator cuff—supraspinatus, infraspinatus, subscapularis, and teres minor—may become inflamed or impinged by the acromion, coracoacromial ligament, acromioclavicular joint, and coracoid process [1]. Fibroblastic hyperplasia (tendinosis) may play a role as well. The supraspinatus tendon is the most commonly involved.
Rotator cuff tendinopathy may result from a variety of factors. The tendon or its musculotendinous junction can be “squeezed” along its course from a relatively narrowed space [2]. Tendinosis can be a result of degeneration from the aging process or from underlying subtle instability of the humeral head [3,4].
In chronic rotator cuff tendinopathy, the muscles of the rotator cuff and surrounding scapulothoracic stabilizers may become weak by disuse. Under these conditions, the muscles can fatigue early, resulting in altered biomechanics. The humeral head moves excessively off the center of the glenoid, usually superiorly [5-8]. From this abnormal motion, impingement of the rotator cuff occurs, causing inflammation of the tendon. This is what many refer to as impingement syndrome; it particularly occurs during forward flexion when the anterior portion of the acromion impinges on the supraspinatus tendon.
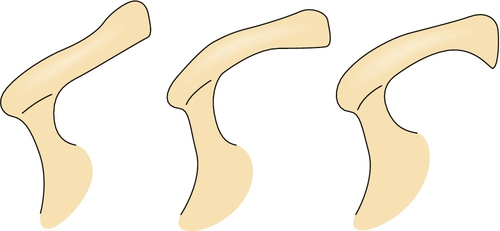
With the passage of time, modifications of the acromion occur, resulting in osteophyte formation or “hooking” of the acromion (Fig. 16.1) [1,9]. With repeated superior migration and acromial changes, degeneration of the musculotendinous junction can lead to tearing of the rotator cuff (see Chapter 17). With prolonged shoulder pain, adhesive capsulitis can develop from the lack of active motion (see Chapter 11).
Symptoms
Patients normally present with pain in the posterolateral shoulder region and, often, deltoid muscle pain, which is referred from the shoulder. The pain is described as dull and achy and often occurs at night. Complaints occur with activities above the shoulder level, usually when the arm is abducted more than 90 degrees. Pain is also noted in movements involving eccentric contractions, when sleeping on the affected side, and during overhead activities such as swimming and painting [10-14].
Physical Examination
The shoulder examination is approached systematically in every patient. It includes inspection, palpation, range of motion, muscle strength testing, and performance of special tests of the shoulder as clinically indicated.
The examination begins with observation of the patient during the history portion of the evaluation. The shoulder should be carefully inspected from the anterior, lateral, and posterior positions. Because shoulder pain is usually unilateral, comparison with the contralateral shoulder is often useful. Atrophy of the supraspinatus and infraspinatus muscles can be seen in massive rotator cuff tears as well as in entrapments of the suprascapular nerve. Scapular winging is rare in rotator cuff injuries; however, abnormalities of scapulothoracic motion are often present and should be addressed as part of the treatment plan.
Tenderness is often localized to the greater tuberosity, subacromial bursa, or long head of the biceps.
Total active and passive range of motion in all planes and scapulohumeral rhythm should be evaluated. Maximal total elevation occurs in the plane of the scapula, which lies approximately 30 degrees forward of the coronal plane. Patients with rotator cuff tears tend to have altered scapulothoracic motion during active shoulder elevation. Decreased active elevation with normal passive range of motion is usually seen in rotator cuff tears secondary to pain and weakness. When both active and passive range of motion is similarly decreased, this usually suggests the onset of adhesive capsulitis. Glenohumeral internal rotation is assessed most accurately by abduction of the shoulder to 90 degrees and manual fixation of the scapula. From this point, the elbow is flexed to 90 degrees and the humerus is internally rotated. The impingement syndrome associated with rotator cuff injuries tends to cause pain with elevation between 60 and 120 degrees (painful arc), when the rotator cuff tendons are compressed against the anterior acromion and coracoacromial ligament [5,6,15].
Muscle strength testing should be done isolating the relevant individual muscles. The anterior cuff (subscapularis) can be assessed by the lift-off test (see Chapter 14, Fig. 14.1), which is performed with the arm internally rotated behind the back. Lifting of the hand away from the back against resistance tests the strength of the subscapularis muscle. The posterior cuff (infraspinatus and teres minor) can be tested with the arm at the side and the elbow flexed to 90 degrees. Significant weakness in external rotation will be seen in large tears of the rotator cuff. The supraspinatus muscle is specifically tested by abduction of the patient’s arm to 90 degrees, horizontal adduction to 20 to 30 degrees, and internal rotation of the arm to the thumbs down position. Testing of the scapula rotators, the trapezius, and the serratus anterior is also important. The serratus anterior can be tested by having the patient lean against a wall; winging of the scapula as the patient pushes against the wall indicates weakness [15,16].
Drop Arm Test
The clinician abducts the patient’s shoulder to 90 degrees and then asks the patient to slowly lower the arm to the side in the same arc of movement. The test result is positive if the patient is unable to return the arm to the side slowly or has severe pain when attempting to do so. A positive result indicates a tear of the rotator cuff [17].
Impingement Sign
The shoulder is forcibly forward flexed with the humerus internally rotated, causing a jamming of the greater tuberosity against the anterior inferior surface of the acromion. Pain with this maneuver reflects a positive test result and indicates an overuse injury to the supraspinatus muscle and possibly to the biceps tendon (see Chapter 14, Fig. 14.2) [18].
Apprehension Test
The arm is abducted 90 degrees and then fully externally rotated while an anteriorly directed force is placed on the posterior humeral head from behind. The patient will become apprehensive and resist further motion if chronic anterior instability is present (see Chapter 14, Fig. 14.4) [1].
Relocation Test
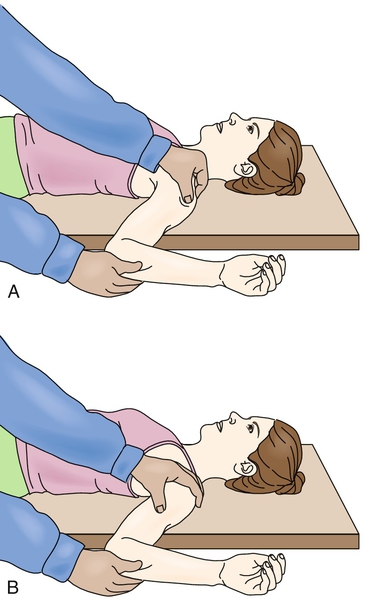
Perform the apprehension test with the patient supine and the shoulder at the edge of the table (Fig. 16.2). A posteriorly directed force on the proximal humerus will cause resolution of the patient’s symptoms of apprehension, which is another indicator of anterior instability (see Chapter 14, Fig. 14.3) [1].
Functional Limitations
Patients with rotator cuff tendinopathy complain of limitations in the performance of overhead activities, such as throwing a baseball and painting a ceiling, particularly above 90 degrees of abduction [19-21]. Pain may also occur with internal and external rotation and may affect daily self-care activities. Women typically have difficulty hooking the bra in back. Work activities, such as filing, hammering overhead, and lifting, can be affected [22,23]. The patient can be awoken by pain in the shoulder, which impairs sleep [12].






