CHAPTER 155
Spinal Cord Injury (Cervical)
Definition
Cervical spinal cord injury (SCI) results in tetraplegia. The term tetraplegia (preferred to quadriplegia) refers to an impairment or loss of motor or sensory function in the cervical segments of the spinal cord due to damage of neural elements within the spinal canal [1]. The result is impairment of function in the arms as well as in the trunk, legs, and pelvic organs. Impairment of sensorimotor involvement outside the spinal canal, such as brachial plexus lesions or injury to peripheral nerves, should not be referred to as tetraplegia.
In a complete cervical SCI, sensory or motor function is absent in the lowest sacral segments S4-S5 (i.e., no anal sensation or voluntary anal contraction is present). If sensory or motor function is partially preserved below the neurologic level and includes the lowest sacral segments, the injury is defined as incomplete [1,2]. The American Spinal Injury Association Impairment Scale (AIS) is used in grading the degree of impairment (Table 155.1). Central cord syndrome is an incomplete SCI syndrome that applies almost exclusively to cervical SCI. It is characterized by greater weakness in the upper limbs than in the lower limbs and sacral sensory sparing [1].
Table 155.1
American Spinal Injury Association Impairment Scale
| Grade | Category | Description |
| A | Complete | No sensory or motor function is preserved in the sacral segments S4-S5. |
| B | Sensory incomplete | Sensory but no motor function is preserved below the neurologic level including the sacral segments S4-S5. |
| C | Motor incomplete* | Motor function is preserved below the neurologic level, and more than half of key muscles below the neurologic level have a muscle grade less than 3. |
| D | Motor incomplete* | Motor function is preserved below the neurologic level, and at least half of key muscles below the neurologic level have a muscle grade 3 or more. |
| E | Normal | Sensory function and motor function are normal; the patient may have abnormalities in reflex examination. |
* There must be some sparing of sensory or motor function in S4-S5 segments to be classified as motor incomplete.
SCI primarily affects young men. However, the average age at injury has increased from 28.7 years in the 1970s to 41.0 years since 2005, and the proportion of new SCI in adults older than 60 years has increased from 4.7% to 13.2% in the same time period in the national Spinal Cord Injury Model Systems database [3]. Males account for about 80% of injuries. The most common cause is motor vehicle accidents, followed by falls, violence (primarily gunshot wounds), and recreational sporting activities [2,3]. The proportion of injuries due to falls has increased over time. Cervical injuries occur more frequently than thoracic and lumbar injuries and accounted for 56.6% of the SCI database between 2005 and 2008. Since 2005, the most frequent neurologic category at discharge reported to the database is incomplete tetraplegia (40.8% of all SCI).
Symptoms
Primary symptoms of cervical SCI are related to muscle paralysis, sensory impairment, and autonomic impairment (including bladder, bowel, and sexual dysfunction). The patient can present in the outpatient setting with a multitude of secondary conditions [4] and associated problems. Symptoms may be vague and nonspecific. For example, urinary tract infections may be manifested not with classic symptoms of urgency and dysuria but with increased spasticity, increased frequency of spontaneous voiding, and lethargy [5]. The patient with pneumonia may present with fever, shortness of breath, or increasing anxiety. Headache may be indicative of autonomic dysreflexia and may be the primary or only presentation of a variety of pathologic processes ranging from bladder distention, urinary infection, constipation, or ingrown toenail to myocardial infarction or acute abdominal emergencies [6]. Table 155.2 lists common presenting symptoms of autonomic dysreflexia and underlying causes.
Table 155.2
Etiology of Common Symptoms in Spinal Cord Injury
| Symptom | Possible Cause |
| Fever | Infectious Urinary tract infection Pneumonia Infected pressure ulcer, cellulitis, osteomyelitis Intra-abdominal or pelvic infection Hot environment (due to poikilothermia) Deep venous thrombosis Heterotopic ossification Pathologic limb fracture Drug fever (e.g., from antibiotics or anticonvulsant pain medications) |
| Fatigue | Nonspecific, but could be the only symptom of serious illness Infection Respiratory or cardiac failure Side effect of medications Depression (inquire about associated dysphoric symptoms) |
| Daytime drowsiness | Side effect of medications (e.g., narcotics, antispasticity agents) Nocturnal sleep apnea Ventilatory failure with carbon dioxide retention Depression |
| Shortness of breath | Pneumonia Abdominal distention (e.g., postprandial, obstipation) Pulmonary embolus Ventilatory impairment (can be postural with sitting up if borderline) Cardiac causes |
| Diarrhea | Altered bowel management schedule Clostridium difficile infection Spurious diarrhea with bowel impaction Side effect of medications (antibiotic, excess laxative or stool softener) |
| Rectal bleeding | Hemorrhoids Trauma from bowel care Colorectal cancer |
| Hematuria | Urinary tract infection Urinary stones Traumatic bladder catheterization Bladder cancer |
| Headache | Autonomic dysreflexia; may be associated with any noxious stimulus below injury level Consider other causes in absence of increased blood pressure |
| Increased spasticity | Urine infection Pressure ulcer Bowel impaction Any noxious stimulus Syringomyelia |
| Pain | Multiple nociceptive and neuropathic causes (see Table 155.3) |
| Unilateral leg swelling | Osteoporotic fracture of the lower extremity Deep venous thrombosis Heterotopic ossification Cellulitis Hematoma Invasive pelvic cancer |
| New weakness or numbness | Syringomyelia Entrapment neuropathy (median at wrist, ulnar at elbow) |
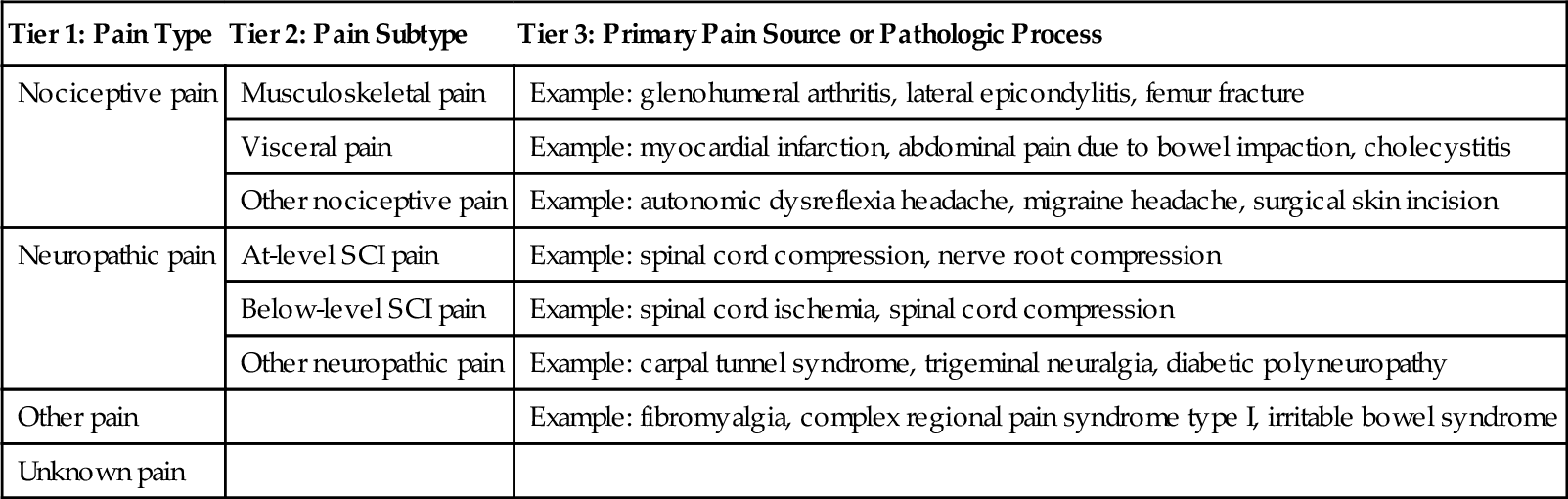
Because symptoms can reflect a variety of underlying conditions, these need to be evaluated carefully. For example, pain in cervical SCI may be multifactorial and needs to be further assessed by characteristics reported in the history, including quality, location, onset, timing, relieving and exacerbating factors, and associated symptoms. Various SCI pain classification systems have been described. The International Spinal Cord Injury Pain classification (Table 155.3) organizes SCI pain into three tiers: tier 1 classifies pain type as nociceptive, neuropathic, other, and unknown; tier 2 includes various subtypes for neuropathic and nociceptive pain; and tier 3 is used to specify the primary pain source or pathologic process [7].
Physical Examination
The neurologic examination is conducted by systematic examination of the dermatomes and myotomes (Tables 155.4 and 155.5) in accordance with the International Standards for Neurological and Functional Classification of Spinal Cord Injury, published by the American Spinal Injury Association [1]. Depending on the presentation, specific elements of the physical examination of various body systems that are relevant in evaluation of SCI-related conditions may include the following.
Table 155.4
Key Sensory Points for Cervical Spinal Segments
| Level | Key Sensory Point |
| C2 | Occipital protuberance |
| C3 | Supraclavicular fossa |
| C4 | Top of the acromioclavicular joint |
| C5 | Lateral side of the antecubital fossa |
| C6 | Thumb, dorsal surface, proximal phalanx |
| C7 | Middle finger, dorsal surface, proximal phalanx |
| C8 | Little finger, dorsal surface, proximal phalanx |
| T1 | Medial side of antecubital fossa |
Table 155.5
Key Muscle Groups for Cervical Myotomes*
| Level | Muscle Group | Positions for Testing Key Muscles for Grades 4 and 5 |
| C5 | Elbow flexors (biceps, brachialis) | Elbow flexed at 90°, arm at patient’s side, forearm supinated |
| C6 | Wrist extensors (extensor carpi radialis longus and brevis) | Wrist in full extension |
| C7 | Elbow extensors (triceps) | Shoulder in neutral rotation, adducted, and in 90° of flexion, with elbow in 45° of flexion |
| C8 | Finger flexors (flexor digitorum profundus) to the middle finger | Full-flexed position of the distal phalanx with the proximal finger joints stabilized in extended position |
| T1 | Small finger abductors (abductor digiti minimi) | Full-abducted position of the fifth digit of the hand |
* For those myotomes that are not clinically testable by manual muscle examination (e.g., C1 to C4), the motor level is presumed to be the same as the sensory level.
Neurologic
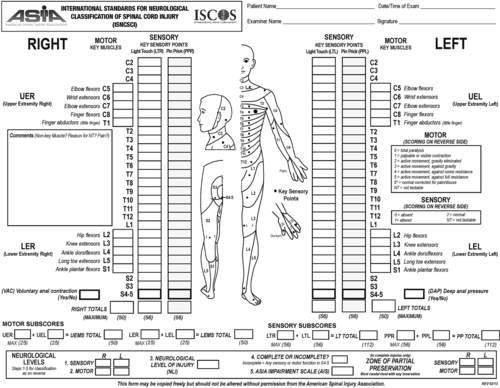
• Determine the level and completeness of the injury (Fig. 155.1). Conduct the examination in the supine position.
• Sensory examination for pinprick and light touch sensation in key points bilaterally (see Table 155.4)
• Motor examination for strength in key muscle groups bilaterally (see Table 155.5)
• Neurologic rectal examination (voluntary anal contraction, deep anal sensation)
• Determine completeness of injury and AIS grade (see Table 155.1). If the AIS grade is A, determine the zone of partial preservation.
• Additional elements of the neurologic examination include
• Position and deep pressure sensation, testing of additional muscles
• Muscle tone and spasticity
• Muscle stretch reflexes, bulbocavernosus reflex, plantar reflex
Respiratory
• Assess respiratory effort, including effect of posture (e.g., sitting versus supine).
• Check for paradoxical respiration and chest expansion.
• Auscultate to assess for decreased breath sounds, rales, and wheeze.
Cardiac
• Low baseline blood pressure is often a “normal” finding in SCI.
• Look for orthostatic symptoms or excess fall in blood pressure with sitting or upright position.
• High blood pressure may indicate autonomic dysreflexia (Table 155.6).
• Examination of peripheral pulses may be especially important for identification of peripheral vascular disease in the absence of claudication and pain symptoms.
Abdomen
• Examine for abdominal distention; examine bowel sounds for evidence of ileus.
• Perform anorectal examination for hemorrhoids and fissures.
Spine
• Identify spinal deformity and tenderness.
• Observe spinal precautions if the examination is being conducted in the acute or postoperative state.
Extremities
• Examine for range of motion, contractures, and swelling.
• Identify nociceptive sources of pain; palpate for tenderness.
• Differentiate effects of SCI (pedal edema, cool extremities) from additional pathologic processes.
Skin
• Examine bone prominences for erythema or skin breakdown.
• Describe any pressure ulcers: location, appearance, size, stage, exudate, odor, necrosis, undermining, sinus tracks; evidence of healing in form of granulation and epithelialization; wound margins and surrounding tissues [8].
Functional Limitations
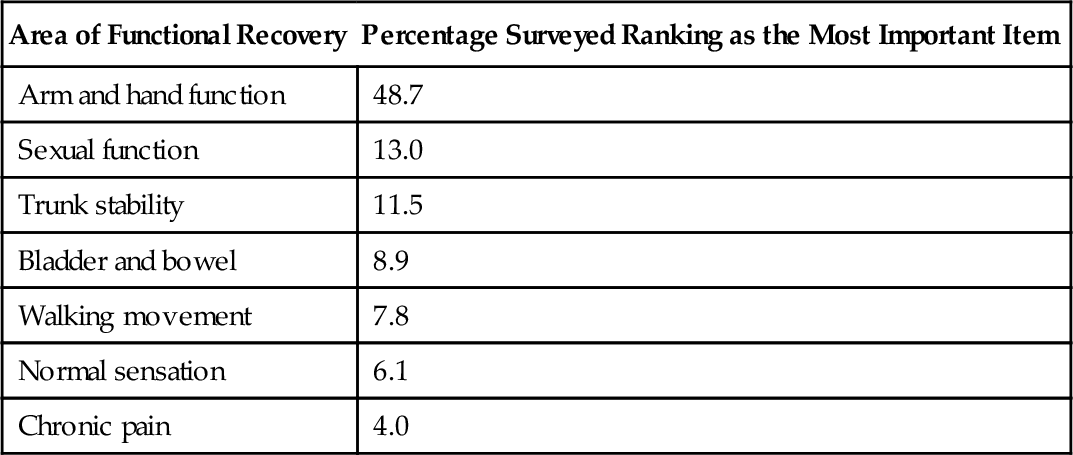
Tetraplegia is associated with several functional limitations based on the level and completeness of injury [9]. Additional factors, such as age, comorbid conditions, pain, spasticity, body habitus, and psychosocial and environmental factors, can affect function after cervical SCI. A survey of individuals with tetraplegia conducted to rank seven functions in order of importance to their quality of life revealed that the greatest percentage ranked recovery of arm and hand function as their highest priority [10] (Table 155.7).
The Consortium for Spinal Cord Medicine has developed clinical practice guidelines on outcomes after SCI with expected functional outcomes for each level of injury in a number of domains [9,11]. Expected functional outcomes and equipment needs for each level of complete cervical SCI are summarized in Tables 155.8 and 155.9.






