26. Neurologic Disorders *
M. Terese Verklan and Suzanne M. Lopez
The developing nervous system provides ongoing challenges for researchers and clinicians. Investigations continue in a wide variety of areas, yet basic mechanisms for a pathophysiologic understanding of common events such as neonatal seizures and intraventricular hemorrhages (IVHs) remain unclear.
Improved neonatal care in recent years has not significantly reduced neurologic sequelae. How much of this is a reflection of survival of sicker and more immature infants is difficult to assess. Primary neurologic disease and secondary neurologic complications from such common conditions as cardiopulmonary disease, metabolic derangements, shock, infection, and coagulopathy still represent major problems encountered in every intensive care nursery. Serious anomalies still appear with regularity, yet in small numbers.
This chapter deals with selected topics in neonatal neurology, including congenital malformations, trauma, seizures, hypoxic-ischemic encephalopathy, and IVH.
CONGENITAL MALFORMATIONS
Physiology, Etiologic Factors, and Clinical Features
Congenital malformations of the nervous system occur when the usual sequence of maturation and development is interrupted (Table 26-1). 39 Present at birth, the etiology is multifactorial and sometimes unclear. Although strictly destructive lesions (e.g., hydranencephaly resulting from bilateral carotid artery occlusion) are separate from primary failures of morphogenesis, both may be included in the broad category of congenital malformations. The distinction between the two types lies in an understanding of the causes.
| Maturational Process | Time | Associated Defects |
|---|---|---|
| Neural tube defects (dorsal induction, neurulation) | 3-4 weeks |
Craniorhachischisis
Anencephaly
Myeloschisis
Encephalocele
Myelomeningocele
Arnold-Chiari malformation
|
| Prosencephalic development61 | 2-3 months |
Cyclopia
Holoprosencephaly
Arrhinencephaly
Septo-optic dysplasia
Agenesis of corpus callosum
Agenesis of septum pellucidum
|
| Proliferation | 2-4 months |
Microcephaly
Megalencephaly
Neurocutaneous syndromes (?)
|
| Migration61 | 3-5 months |
Schizencephaly
Lissencephaly
Pachygyria (macrogyria)
Microgyria (polymicrogyria)
Neuronal heterotopias
|
| Neuronal organization and functional organization | 6 months |
Down syndrome (?)
Mental retardation (?)
Genetic epilepsy (?)
|
| Myelination61 | 2nd trimester61 | Anoxic/ischemic damage |
Understanding congenital malformations requires an appreciation of the normal embryologic sequence. 39 The clinical and pathologic identification of normal and abnormal structures makes it possible to determine the timing of the insult or development failure. Once timing is established, an appropriate search for the cause can be made.
Neural Tube Defects
The incidence in the United States of neural tube defects (NTDs) is approximately 1 to 2 in 1000 births (see the Critical Findings box on p. 749). 41 Although the prevalence of NTDs has decreased, they are one of the most common congenital anomalies contributing to morbidity and mortality in neonates. 2 Changes in vertebral, vascular, meningeal, and dermal structures are typically found along with the defects. The more common types of NTDs include anencephaly, encephalocele, myelomeningocele, and occult spina bifida. 5 Genetic and environmental factors play a role in the development of NTDs. Familial incidence also plays a role; when one family member is affected, the risk increases by 2% to 3% in subsequent offspring and doubles if two or more family members are affected. 5 Cytogenic abnormalities are found in approximately 2% to 16% of neonates who have an isolated NTD. 35 Teratogen exposure has also been linked to NTDs. 39 A prepregnancy history of diabetes, specific drugs (especially anticonvulsants and sulfonamide drugs), and maternal hyperthermia secondary to using a hot tub or sauna have been identified as risk factors. 17 Recently, prepregnancy maternal obesity also has been linked to an increased risk. 64
The major environmental factor linked to NTDs is a dietary level of folic acid. 27 Folic acid supplements before and during pregnancy have been cited as substantially lowering the incidence of these NTDs. The U.S. Public Health Service issued a recommendation that women of childbearing years consume 400 mcg of folic acid each day to prevent NTDs. The American Academy of Pediatrics (AAP) also supports this recommendation. 9,16,27,39,41 Such an intake can be achieved by dietary supplementation of folate, adding folic acid to U.S. enriched grain products (e.g., bread, flour), and consuming foods containing folic acid (e.g., citrus fruit, beans, leafy greens). The Food and Drug Administration (FDA) required all enriched grain products to be fortified with folic acid by 1998. 6,16 In spite of this, it has been reported by the Centers for Disease Control and Prevention (CDC) that two thirds of American women fail to ingest an adequate amount of folic acid. 9 It has been argued that the amount of folic acid supplementation in grain products may be inadequate, supplying only about one fourth of daily need. 40 Noting the 26% decrease in the incidence of NTDs after the FDA required 140 mcg folic acid per 100 g of grain, the March of Dimes recommended an increase in the level of folic acid fortification. 37,62 Others, including the CDC and AAP, concur with this recommendation to increase the requirement to 350 mcg folic acid per 100 g of grain. 7
Neural Tube Defects
• As many as 50% or more of neural tube defects (NTDs) are preventable.
• Two thirds of American women fail to ingest an adequate amount of folic acid, and enriched grain products supply only one fourth of daily need.
• All women of childbearing age should consume 400 mcg of folic acid daily even when not planning to become pregnant.
• At increased risk: women with a prior NTD pregnancy. For these women, the recommended dose of folic acid is increased to 4 mg daily. It should be taken at least 1 month before conception.
• Sources: Dietary supplements, enriched grain products, and consumption of foods with folic acid content (citrus fruit, beans, leafy greens).
• The Centers for Disease Control and Prevention (CDC,) the American Academy of Pediatrics (AAP), and the March of Dimes have all recommended an increase in the amount of folic acid used to fortify grain products from 140 mcg to 350 mcg per 100 g of grain.
• Inadequate education of women continues to be a problem.
A Cochrane review concluded that supplementation of folate provides “a strong protective effect against neural tube defects.” Recommendations were made to increase availability of information about folate. Another recommendation was to advise women with a prior NTD pregnancy of the increased risk for future pregnancy and to provide them with folate supplementation. 34 For women with a prior NTD pregnancy, the recommended dosage of folic acid is increased to 4 mg daily, which should be taken for at least 1 month before conception. 6,16,20 Unfortunately, it has been reported that some health care providers in contact with women of childbearing age are not counseling them about the importance of folic acid consumption or the appropriate amount to take. 20 It should not be expected that an improved consumption of folic acid will totally prevent all NTDs because of etiologic factors such as the environment and genetics.
At the end of the first embryonic week, the primitive streak is present on the rostral surface of the embryo. A second streak, the notochordal process, develops alongside the primitive streak. The notochord is responsible for the induction of both the neural plate and the neurenteric canal. Cells proliferate along the lateral margin of the neural plate to form the neural folds around the central neural groove. 61
Cells at the apex of the neural folds make up the neural crest. Schwann cells, pia-arachnoid cells, sensory ganglia, melanocytes, and various secretory cells arise from the neural crest. The neural folds meet and fuse with the rostral (anterior) and caudal (posterior) ends (neuropore), closing by approximately the end of the fourth embryonic week. 61
Failure of development at this stage results in the defects of neurulation (or dorsal induction). The most severe of these defects is craniorachischisis, in which there is significant malformation of the brain (as in anencephaly), absence of the posterior skull, and an open spine along the full length of the spinal cord. Only a few affected embryos survive to early fetal stages. 61
Anencephaly is similar to craniorachischisis without the spinal defect. There is essentially no normal brain tissue above the brainstem and thalami, and parts of those structures are malformed. Onset is thought to occur before 24 days’ gestation. About one fourth of the fetuses survive into the neonatal period, but three fourths are stillborn. The majority of anencephalic infants die within the first week of life without intensive care. 61
Myeloschisis involves the failure of the posterior neural tube to close. There is no well-defined sac protruding from the defect. 8
Encephaloceles are caused by a limited failure of closure at the rostral (head) end of the neural tube. Extensions of meninges or brain tissue through the skull may occur on the ventral or rostral surface. 61
Myelomeningoceles (or even the more limited meningoceles) are a limited form of myeloschisis with failure of closure at the caudal (tail) end of the neural tube. With meningocele, the meninges protrude through the vertebrae and are contained within a sack. The spinal cord and nerve roots are generally in normal position, which improves the outcomes for these children. Unfortunately, myelomeningoceles, the more common defect, result in protrusion of both meninges and spinal cord through the opening in the spinal column. Neurologic deficits occur below the level of the protrusion. 35,47,56 The Arnold-Chiari deformities usually are included here. These malformations, often seen with myelomeningoceles, involve structures of the brainstem and cerebellum. Generally, the cerebellar tonsils are pulled down through the foramen magnum, and the brainstem is elongated in later life. Hydrocephalus is common. Dilation of ventricles often occurs without increased head circumference or clinical symptoms of increased intracranial pressure in this group of infants; therefore serial computed tomography (CT) or ultrasonographic scans should be performed. Symptoms of brainstem involvement may be present. Open myelomeningoceles and anencephaly (any defect in which the spinal or cranial contents are “open” to the outside) are associated with an elevation of alpha fetoprotein (AFP) in the amniotic fluid. This is important in prenatal diagnosis. 61
Segmentation Defects
After formation and closure of the neural tube, the development of the different regions of the brain begins to occur. Suprasegmental structures are formed. The division of the brain into hemispheres, formation of the ventricular system, and formation of the major gyral patterns are all part of this period of development. Major areas of the brain, including the cerebellum, basal ganglia, brainstem nuclei, thalamus, and hypothalamus, form at this time. 61 Defects of segmentation and cleavage occur during this phase of neural development. For unknown reasons, defects of segmentation and cleavage are far less common than defects of neurulation. Because these malformations involve abnormalities of ventral induction rather than dorsal induction (e.g., neurulation), the face, eyes, nose, mouth, and hair are also involved in the malformation. These features always should be investigated carefully for specific anomalies.
Holoprosencephaly is characterized by a single midline lateral ventricle, incomplete or absent interhemispheric fissure, absent olfactory system, midfacial clefts, and hypotelorism. The most severe form of holoprosencephaly is cyclopia (a single fused midline eye) and supraorbital nasal structure. At times, the nasal structure and eye are absent. An intermediate form is cebocephaly, which includes ocular hypotelorism (abnormally decreased space between the eyes) and a flat nose with single nostril. 61
When any of these malformations are suspected or when features suggestive of them are seen, careful examination of the hair, eyes, ears, mouth, and nose may reveal other related anomalies.
Migration and Cortical Organizational Defects
A critical aspect of brain development has yet to be described. The remaining development of the brain takes over twice as long as previously described development and includes cellular proliferation, migration, organization, and myelination. Cells that later form the cerebral cortex begin in the germinal matrix (near the caudate nucleus around the lateral ventricles). These cells then migrate in a radial fashion to their final positions near the surface of the brain. Abnormalities of cellular migration result in collections of gray matter in unusual places (heterotopias), abnormal gyri and sulci, abnormal spaces in the brain, and frequent clinical signs of gray matter dysfunction. Frequently, these clinical problems are not apparent in the newborn period.
Microcephaly means “small brain” and is manifested as a head circumference measuring greater than two standard deviations below average for infants at that gestational age. 17 Microcephaly may be (1) genetic (dominant, recessive, sex-linked) or chromosomal (translocation [see Chapter 27]); (2) caused by teratogens (cocaine, alcohol); (3) caused by infection (rubella, cytomegalovirus); or (4) of unknown cause. Occasionally there is a paucity of germinal matrix cells or they fail to adequately migrate, resulting in a brain cortex with a decreased number of neuronal cells. 61
In lissencephaly, the brain is smooth in appearance, having little or no gyri (convolutions). Although not generally present at birth, microcephaly usually occurs within the first year in type I lissencephaly. Appearance is marked by hollowing at both temples, a small jaw, and hypotonia. Neonatal seizures may be present, but seizures are more commonly present at 6 to 12 months of age. Another form of type I lissencephaly is Miller-Dieker syndrome, in which craniofacial deviations occur. In type II lissencephaly, macrocephaly is generally present at birth or develops soon afterward. Retinal, cerebellar, and muscular abnormalities always are present. 61
Clinical features of lissencephaly include seizures, microcephaly, hypotonia, feeding problems, scarcity of movement, upturned nares, temporal hollows, small jaw, protruding and long upper lip, and abnormalities on the electroencephalogram (EEG). Later, mental retardation and severe spasticity may be noted and death may occur. 61
Additional Defects
Cerebellar malformations are quite varied. Most often, at least a portion of the cerebellum is preserved, but total absence is possible. Hemispheric aplasia or vermal aplasia is seen, and familial forms have been reported. The Dandy-Walker cyst is another complex malformation involving the cerebellum in which the fourth ventricle is dilated into a cystic structure. The foramina of Magendie and Luschka are atretic, and hydrocephalus results. The cerebellum is small and displaced upward. Associated anomalies include heterotopias, agenesis of the corpus callosum, aqueductal stenosis, and syringomyelia. Causation is unknown. The differential diagnosis includes an arachnoid cyst of the posterior fossa. In the case of an arachnoid cyst, the fourth ventricle is not part of the malformation and is normal, although it may be displaced. 61
Clinical features of the Dandy-Walker cyst include frequent progressive hydrocephalus, associated malformations that cause additional specific symptoms, possible absence of symptoms in the newborn period, enlargement of the occipital shelf and posterior part of the skull, and clinical symptoms of increased intracranial pressure. 61
Craniosynostosis is the abnormally early closure (fusion) of the bones of the skull. Causation of this malformation is unknown. The premature closure of sutures may involve one or many sutures, with resulting deformity of the skull. Numerous terms are used to describe the shapes the skull assumes when craniosynostosis is present. 61
Craniosynostosis should be suspected in the presence of microcephaly or misshapen head. Appropriate evaluation requires x-ray films of the skull and a CT scan to define which, if any, of the sutures are stenosed and what problems might exist with brain structure (pressure or malformation). 61
Hydrocephalus may occur in many different situations from many separate causes. An inherited X-linked form exists. Intrauterine infection is another cause. Hydrocephalus may be associated with many of the malformations described previously. Hydrocephalus results when the normal flow of ventriculospinal fluid is obstructed. This may be the result of an atretic portion of the ventricular system, blockage from the outside, inflammation within the ventricular system causing a permanent blockage, or (very rarely) overproduction of ventriculospinal fluid. 35,61
Data Collection
The diagnosis of malformations of the central nervous system (CNS) may be quite obvious (as in anencephaly) or more subtle. Careful examination of all newborns results in the identification of most malformations. At times, the diagnosis is suspected not on the basis of findings on examination but because of an accompanying sign, such as seizures. 5
Two very important tests have become available in recent years that allow prenatal diagnosis of certain congenital malformations of the nervous system. Ultrasonographic examination (an abdominal ultrasound scan of the mother) provides an opportunity to identify certain malformations by viewing the fetus during development. Hydrocephalus, encephaloceles, myelomeningoceles, and anencephaly may be identified prenatally. Determination of AFP in the amniotic fluid and maternal serum allows the identification of anencephaly and open myelomeningoceles. A non-enclosed nervous system is associated with a significant rise in AFP in the amniotic fluid. Amniocentesis provides the amniotic fluid necessary for this determination. Testing of maternal serum for AFP also is an option and at some centers may be used along with ultrasonography for diagnosis, allowing amniocentesis to be omitted. 61 Clinical signs and symptoms have been described for each individual nervous system malformation presented earlier in this chapter.
Treatment
Limited treatment is available for congenital malformations of the nervous system. A variety of strategies are available for reducing secondary complications or providing earlier management to handle these complications more efficiently.
The greatest efforts and accomplishments have been made for infants with congenital malformations who might be expected to have productive lives. When secondary complications are managed appropriately, the majority of children with myelomeningoceles are ambulatory (total or partial) and continent of urine. 61
Myelomeningocele generally is surgically repaired as soon as possible (within 24 to 48 hours).5,35,47,61 Prevention of infection is paramount. In addition to sterile technique, prophylactic antibiotics have been shown to be beneficial. 61Trauma to the area should be avoided by keeping the infant in the prone position and maintaining sterile gauze moistened with warm, sterile normal saline. Tape should be avoided. 5,35,44 Preventing fecal contamination is vital. Several authors recommend the use of a sterile, plastic drape fastened above the anus but below the lesion to keep fecal material isolated from the site. 35,44Latex precautions also should be initiated, because these infants have an increased propensity for developing sensitivity to latex.5
In addition, spina bifida has been repaired in utero at early gestational age. Such repairs have risks for both mother and fetus but have resulted in reported significant drops in the number of infants developing hydrocephalus that would require a postnatal ventriculoperitoneal shunt. 15 Because of a lack of improved neurologic outcomes overall, a multicenter randomized controlled trial (RCT) is underway to compare intrauterine therapy to conventional postnatal care to better identify procedure-related benefits and risks. 15
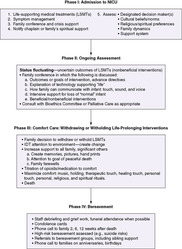
Some of the malformations are lethal very soon after birth (anencephaly), limiting management options for comfort measures and family support. When appropriate, genetic counseling should be requested. For other malformations, treatment requires management of symptoms such as seizures, signs of increased intracranial pressure, and infection. A consult to neurosurgery is indicated. Other helpful consults may include physical therapy, infectious diseases, urology, and orthopedics. 35 For hydrocephalus, shunting may become necessary. See Box 26-1, the Parent Teaching box on pp. 754-755 and Figure 26-1). 61
BOX 26-1
• Positioning:
• Place infant on unaffected side (may position on shunt side with “doughnut” over operative site once incision has healed). Keep head of bed flat (15 to 30 degrees) to prevent too-rapid fluid loss.
• Support head carefully when moving infant.
• Turn q 2 hr from unaffected side of head to back.
• Shunt site:
• Use strict aseptic technique when changing dressing.
• Pump shunt if and only as directed by neurosurgeon.
• Observe for fluid leakage around pump.
• Observe and document all intake and output. Watch for symptoms of excessive drainage of CSF:
• Sunken fontanel
• Increased urine output
• Increased sodium loss
• Observe, document, and report any seizure activity or paresis.
• Observe for signs of ileus:
• Abdominal distention (serially measure abdominal girth)
• Absence of bowel sounds
• Loss of gastric content by emesis or through orogastric tube
• Perform range-of-motion exercises on all extremities.
• Observe and assess for symptoms of increased intracranial pressure (shunt failure):
• Increasing head circumference (measure head daily)
• Full or tense fontanel
• Sutures palpably more separated
• High-pitched, shrill cry
• Irritability and/or sleeplessness
• Vomiting
• Poor feeding
• Nystagmus
• Sunset sign of eyes
• Shiny scalp with distended vessels
• Hypotonia and/or hypertonia
• Observe and assess for signs of infection:
• Redness or drainage at shunt site
• Hypothermia and/or hyperthermia
• Lethargy and/or irritability
• Poor feeding and/or poor weight gain
• Pallor
• Parent teaching:
• Demonstrate and receive return demonstration of drug administration.
• Teach parents side effects of medications.
• Document on NICU’s routine discharge teaching checklist with routine care.
 |
| FIGURE 26-1
(From Harrison H, Kositsky A: The premature baby book, New York, 1983, St Martin’s Press.)
|
The one situation in which microcephaly could be considered surgically treatable is total craniosynostosis. Generally, skull deformity is present in infants with craniosynostosis, and it is always wise to consider the presence of craniosynostosis in any infant with a small head. If present, total craniosynostosis should be treated surgically. 35
The management of congenital hydrocephalus consists primarily of early shunting as soon after birth as possible. Fetal surgery for placement of a ventriculoamniotic shunt has been proposed, but an improvement in outcomes compared with surgery after birth is uncertain. In addition, hydrocephalus in a fetus is often associated with serious developmental abnormalities that may increase morbidity and mortality. 61
In Volpe’s series, outcome was variable and the procedures were not as reliable as hoped. It was not always possible to distinguish true hydrocephalus from ventriculomegaly without increased pressure. Shunting soon after birth often produces a far better outcome than would be assumed, with minimal motor deficit and only a mild to moderate deficit in intellect. 61
Wolfson Children’s Hospital Parent Handout: Newborn Ventriculoperitoneal Shunt (For Use With Ventriculoperitoneal Shunt Teaching Checklist)
Purpose of Ventriculoperitoneal Shunt
• Ventricles are compartment-like spaces that are located in the normal brain. Spinal fluid forms daily in these ventricles. This clear fluid flows out over the brain and down around the spinal cord. Spinal fluid helps cushion the brain from injury, keeps the brain moist, and carries away waste products.
• Hydrocephalus is a condition in which an abnormally large amount of spinal fluid builds up in your baby’s ventricles and usually is caused by a blockage in the spinal fluid path. Because the ventricles continue to make spinal fluid daily, a buildup of fluid occurs when it cannot escape. This excess fluid can cause pressure on the brain and result in permanent damage to the brain unless it is properly treated.
• The purpose and function of your baby’s VP shunt is to allow the excess spinal fluid to drain through a tube from the ventricle into the abdomen, where it is absorbed.
Pathway of the Ventriculoperitoneal Shunt
• A small incision is made on the scalp, and the tube is passed through the skull and into the ventricle. Located under the skin, the tube passes behind the ear, down the side of the neck, and continues to the abdomen, where a second incision is made to put the end of the tube into the abdominal cavity. A third incision is sometimes needed in the neck area with some babies.
• The scalp incision will be hidden as your baby’s hair grows. You will see and feel the shunt tubing (like a large vein under the skin), but it is barely noticeable after the baby gains weight.
Signs and Symptoms of Shunt Infection
• The shunt is at risk for infection because it is a foreign object located inside the body. You will have to watch for these signs of shunt infection and report them immediately to your doctor:
• Temperature of 101° F or higher
• Swelling, redness, or drainage along the pathway of the shunt tube
• Lethargy or irritability (change in behavior)
• Loss of appetite or poor feeding
Signs and Symptoms of Shunt Failure/Increased Intracranial Pressure
• The spinal fluid contains proteins and chemicals that may build up and block off the shunt. It is also possible for tissue within the brain or abdomen to block the shunt or for the shunt device itself to fail. This shunt failure (malfunction) means that the spinal fluid will once again build up and result in pressure on the brain and possible irreversible damage. Therefore it is very important for you to watch for the signs of increased pressure in the brain that occurs with shunt failure and report them to your doctor immediately:
• Lethargy or sleepiness
• Unusual irritability, fussiness, or excessive crying
• Repeated vomiting
• Poor feeding
• Bulging soft spot when baby is sitting up quietly
• Shrill, high-pitched cry
• Eyes that look downward
• Increase in spaces between the bones of the skull
• Seizures/posturing
Reason and Importance of Prompt Treatment of Health Problems
• Prompt treatment of your baby’s health problems (e.g., ear infections, skin infections) is important to prevent infections spreading to the shunt. It is also vital to seek medical care for signs of shunt infection or failure as noted.
Importance of Close Medical Follow-up
• Your baby will have to be followed up by a neurosurgeon and your pediatrician after being discharged. Bring the baby to every follow-up appointment so that your baby’s head can be measured and physical condition can be evaluated. Your baby will also go to the Developmental Evaluation Clinic where a specialist in baby development can examine him or her. If development problems occur, this will ensure early diagnosis and treatment.
Care of the Shunt
• You can handle, cuddle, and play with your baby like any baby. Your baby also can sleep in any position after the initial postoperative period.
 |
Monitoring of pregnancies with fetal ultrasound allows the detection of congenital hydrocephalus. Induction of lung maturation with steroids has been suggested to allow a preterm delivery (with a smaller head) without excessive pulmonary complications. In this way, a permanent shunt can be placed sooner than with term delivery. 61
Complications
Many of the expected complications were dealt with previously in the sections describing the malformations and their associated problems. It is difficult to separate true complications from problems resulting from the malformation. For example, hydrocephalus develops in many infants with myelomeningocele and may be present at birth. 5,47 Other complications or associated problems of myelomeningocele include bowel and bladder incontinence, meningitis, urinary tract infections, and paralysis. 35
Malformations carry with them altered anatomy and physiology that is reflected in abnormal function. Common general problems include seizures, mental retardation, sensorimotor abnormalities, disturbances in primary sensory function such as vision and hearing, orthopedic problems, and vegetative functions. 61
The problems encountered are ordinarily explained on the basis of the malformation. Often midline defects in the brain (particularly at the base of the brain) have clinical problems involving the hypothalamus. Diabetes insipidus may be present.
To some extent, the anatomy predicts the types of problems. Involvement of the cortex causes seizures, retardation, and sensorimotor problems. White matter damage can cause spasticity. If the brainstem is involved in the malformation, apnea, deafness, sleep disturbance, oculomotor disturbances, and problems with sucking and swallowing may be seen. Spinal cord lesions cause quadriplegia or paraplegia. Genitourinary problems and, to a lesser extent, gastrointestinal problems also are seen.
Apnea and other brainstem findings may occur when the malformation involves the brainstem, as in Arnold-Chiari deformity, Dandy-Walker cyst, occipital encephalocele, and arachnoid cyst.
Pituitary-hypothalamic dysfunction may manifest itself in impaired temperature regulation, thyroid abnormalities, diabetes insipidus, and adrenal insufficiency.
Most of the complications occur after the newborn period, although causation is present at birth and includes seizures, retardation, spasticity, genitourinary problems, and orthopedic problems. In many circumstances, the problem is already present but functional expression, such as impaired ambulation, mental retardation, or deafness, is lacking. In the infant’s follow-up examinations, careful attention must be given to problems likely to develop or intensify with age. When a specific malformation is identified, it is necessary to become familiar with the expected problems, not only to anticipate problems as they appear but also to lessen any secondary damage that might occur if they go unrecognized.
Parent Teaching
Parents of an infant born with congenital malformations are faced with a stressful event that may develop into a major life transition. Parents, especially mothers, report feelings of guilt and self-blame, although they may not initially share these feelings with hospital staff. After the birth of a malformed child, they go through stages of grief (see Chapters 29 and 30): shock or denial, anger, bargaining, depression, and acceptance. Some authors question whether full acceptance occurs for the family of the handicapped child because of return of grief and sorrow each time a developmental milestone is missed or the child experiences illness. 38,44
Social support received from hospital personnel, family, and friends can help parents feel less stressed and more able to cope with the illness of their infant. The ability of the staff to accurately anticipate and assess parental feelings and concerns can be invaluable when assisting families through this difficult time. Parents should be encouraged to verbalize their feelings and fears in a supportive environment. Reassurances, when appropriate, should be provided (e.g., parents were not responsible for the congenital malformation; it is normal for the mother to experience [or at least report] more fears than her husband). The ultimate goal of intervention is to reduce stress, assist families to confront fears, improve coping, and facilitate the bonding process.38
Infants with congenital malformations present such a complex variety of problems that parent teaching and emotional support need to begin as early as possible. Often parents know from the time of birth or earlier that a major problem exists. In other circumstances, the anomaly is detected only after appropriate studies are performed.
When the infant is not viable, care should be directed at meeting the emotional needs of the family. Every effort should be made to give family members positive experiences and memories by encouraging early parental holding of the infant and, whenever possible, participation with care (see Chapter 30). Anticipatory counseling from social services and chaplain staff can help the family during grieving and with funeral arrangements. There are also questions about etiologic factors and genetics, and these questions should be dealt with according to the family’s wishes (see Chapter 27).
If serious handicaps are anticipated and the infant is expected to survive, the parents should be encouraged to participate in the care of the infant from the beginning. Both adjustment and specific aspects of care within the circumstance will be enhanced and learning will be more effective if parents are supported. A multidisciplinary team approach to parent education and support allows individualized hospital resources for specific needs of the patient and family. In addition to medical, nursing, social service, and chaplain involvement, team members can be drawn from psychology, developmental specialists, physical therapy/occupational therapy, and other services based on specific needs and circumstances. Parent teaching and support must be individualized according to the anomaly. When available, support groups, integrative discharge planning, and specialized clinics can help with post-discharge care and parent education.
Parent teaching for the mothers and fathers of infants with congenital anomalies should (1) be started early, (2) involve the parents in the care of the infant, (3) use the resources of the hospital for specialized help, and (4) continue after the infant has gone home from the hospital. 38
BIRTH INJURIES
Physiology and Etiology
Birth injuries (birth traumas) are the direct result of difficulties encountered during the delivery process. These may be minor injuries without expected sequelae or the direct cause of death in the neonatal period. Classification of birth injuries usually is etiologic (predisposing factors or mechanisms of injury) or anatomic. An anatomic classification is used in this discussion to illustrate commonly encountered problems (Table 26-2).
| Site of Injury | Type of Injury |
|---|---|
| Scalp |
Caput succedaneum
Subgaleal hemorrhage
Cephalhematoma
|
| Skull |
Linea fracture
Depressed fracture
Occipital osteodiastasis
|
| Intracranial |
Epidural hematoma
Subdural hematoma (laceration of flax, tentorium, or superficial veins)
Subarachnoid hemorrhage
Cerebral contusion
Cerebellar contusion
Intracerebellar hematoma
|
| Spinal cord (cervical) |
Vertebral artery injury
Intraspinal hemorrhage
Spinal cord transection or injury
|
| Plexus injuries |
Erb’s palsy
Klumpke’s paralysis
Total (mixed) brachial plexus injury
Horner syndrome
Diaphragmatic paralysis
Lumbosacral plexus injury
|
| Cranial and peripheral nerve injuries |
Radial nerve palsy/nerve injuries
Medial nerve palsy
Sciatic nerve palsy
Laryngeal nerve palsy
Diaphragmatic paralysis
Facial nerve palsy
|
The timing of birth injuries can be used to identify and describe causes. Etiologic classification of birth injuries includes uterine injury (antenatal), fetal monitoring procedures, abnormal or difficult presentations or methods of delivery, and multifactorial injuries. It should be recognized that the same injury might have multiple causations. Thus a cephalhematoma could be the result of forceps delivery, vacuum extraction, or routine vaginal delivery. A variety of specific predisposing factors increase the risk for birth injury, as follows:
• Macrosomia
• Cephalopelvic disproportion
• Dystocia
• Prematurity
• Prolonged or precipitous labor
• Breech presentation
• Forceps usage
• Rotation of fetus
• Version and extraction
• Handling after delivery
Multiple factors often are present. When multiple predisposing factors are present, a single underlying maternal disease often links them. A common example is that of a premature, macrosomic fetus with a diabetic mother in whom labor is not progressing properly.
The common factors that are present in deliveries complicated by birth injuries are as follows:
• Unusual progress of labor
• Unusual size or shape of the fetus (large for gestational age or hydrocephalus)
• Problems encountered during delivery (dystocia or forceps application)
• Unusual or unexpected presentations (breech or unexpected twin)
The maternal history must always be explored for the underlying disease process or conditions that might increase the risk for a birth injury.
Prevention
Most birth injuries may be preventable, at least in theory. Careful attention to risk factors and the appropriate planning of delivery should reduce the incidence of birth injuries to a minimum. Transabdominal ultrasonography facilitates predelivery awareness of macrosomia, hydrocephalus, and unusual presentations. Particular pregnancies then may be delivered by controlled elective cesarean section to avoid significant birth injury. Care must be taken to avoid substituting a procedure of greater risk. Often a small percentage of significant birth injuries cannot be anticipated until the specific circumstances are encountered during delivery. Emergency cesarean section may provide last-minute salvage, but in these circumstances, the injury truly may be unavoidable.
SPECIFIC BIRTH INJURIES
Injuries to the Scalp
The three commonly encountered forms of extracranial hemorrhage are caput succedaneum, subgaleal hemorrhage, and cephalhematoma and are distinguished not only in clinical manifestations but also in pathophysiology (see the Critical Findings box at right. 61 These three extracranial scalp injuries are included with neurologic birth injuries, not because they have associated neurologic problems but because the family or health care providers often raise the question of possible neurologic involvement.
Extracranial Hemorrhage
There are three common forms of extracranial hemorrhage but with different etiology and clinical assessment findings, as follows.
1. Caput succedaneum
a. Etiology: Trauma to scalp (usually vertex vaginal delivery) results in hemorrhagic edema superficial to the aponeurosis of the scalp.
b. Findings: Soft, pitting edema that crosses suture lines.
2. Cephalhematoma
a. Etiology: Mechanical trauma; most common in primiparous women, with delivery using forceps or in vacuum-assisted deliveries.
b. Findings: Firm, tense collection of blood confined by the sutures. Area often increases in size after delivery. No significant blood loss. Blood collects beneath the periosteum (subperiosteal).
c. Warning: Associated with linear skull fracture in up to 25% of the cases.
3. Subgaleal hemorrhage
a. Etiology: Forces that compress and then drag head through pelvic outlet.
b. Findings: Firm swelling that crosses suture lines and is fluctuant to palpation. Blood collection is under the aponeurosis (connective tissue connecting the occipital and frontal muscles). Bleeding (swelling) may continue after birth and dissect along tissue planes into the neck.
c. Warning: Acute blood loss may occur. Presenting symptom may be shock.
Monitor VS for signs of shock:
Elevated HR
Decreasing BP
Monitor baby for signs of shock:
Pallor
Delayed capillary refill time
Diminished tone
Respiratory distress
Transfusion may be necessary: type and crossmatch.
Serial Hct should be followed.
Elevated bilirubin is a common complication as a by-product of broken-down red blood cells.
PHYSIOLOGY AND ETIOLOGY
Caput succedaneum is caused by trauma to the scalp, usually during a routine vertex vaginal delivery. The caput is the result of hemorrhagic edema superficial to the periosteum of the scalp. Therefore spread of the edema is not restricted to suture lines and is soft and pitting because of its superficial location. 35,61
Forces that compress and drag the head through the pelvic outlet are associated with subgaleal hemorrhage. Significant acute blood loss can occur with shock as the presenting symptom. Bleeding may continue after birth with enlargement of the accumulated blood and dissection of the blood along tissue planes into the neck. Such a hemorrhage carries the greatest potential for complications, but fortunately it is the least common form of birth injury to the scalp. 32,35,61
Cephalhematoma is a subperiosteal collection of blood that is confined by the skull sutures. The incidence is 1% to 2% of all live births. The cause is nearly always mechanical trauma, and its occurrence is more common in primiparous women and in forceps or vacuum-assisted delivery. Males are generally more likely to be affected than females. It is associated with an underlying linear skull fracture in up to 25% of cases. The firm, tense collection of blood frequently increases in size after birth, but significant blood loss does not occur. 5,35,61
DATA COLLECTION
With caput succedaneum, physical examination reveals soft, pitting edema that is diffuse and crosses suture lines. Laboratory tests are not needed. 35,61
Because the subgaleal collection of blood is under the aponeurosis (connective tissue connecting the occipital and frontal muscles) and superficial to the periosteum, subgaleal hemorrhage crosses suture lines. It is firm but fluctuant to palpation. Vital signs should be carefully monitored for symptoms of shock. Pallor, delayed capillary refill time, diminished tone, respiratory distress, elevated heart rate, or decreasing blood pressure should be observed for and treated promptly. Transfusion may be necessary. The hematocrit should be serially followed, and bilirubin levels should be determined during recovery.35,61
Cephalhematomas may occur anywhere but are most commonly found in the parietal area on one side. Because the location of the blood is subperiosteal, the blood is confined by suture lines. Symptoms are normally absent. A skull fracture underlying the cephalhematoma is present in 10% to 25% of affected infants. X-ray examination of the skull defines the fracture. Rare complications include infection, osteomyelitis, hyperbilirubinemia, meningitis, and late-onset anemia. 35,61
TREATMENT
Usually, no treatment is necessary for any of these three lesions. In subgaleal hemorrhage, treatment of blood loss and shock may be necessary. During resolution, the breakdown of the blood may cause hyperbilirubinemia requiring treatment (see Chapter 21). 35,61
PARENT TEACHING
Parents of an infant with caput succedaneum should understand that the swelling is outside of the cavity of the brain and will usually reabsorb within 48 hours. 35Careful preparation of the parents for the acute side effects of subgaleal hemorrhage is important. Parents should be warned of the possibility of swelling and discoloration of the face, head, and neck. The purpose of serial hematocrit and bilirubin checks should be explained. Parents can expect 2 to 3 weeks for the swelling to resolve. 35 Parents of an infant with a cephalhematoma should be instructed that the cephalohematoma may enlarge but that they should not be concerned unless localized changes occur, suggesting secondary infection (erythema, induration, or drainage). This lesion should not be drained and may be evident for 6 to 8 weeks and leave a small calcification after reabsorption of hemorrhage. The hemorrhage can be significant enough to cause hyperbilirubinemia or anemia. Outpatient evaluation of bilirubin levels and hematocrit may be needed in some cases.
Skull Fractures
Three forms of skull fracture should be identified and differentiated: linear fractures, depressed fractures, and occipital osteodiastasis. 35,61
PHYSIOLOGY AND ETIOLOGY
Linear skull fracture (a nondepressed fracture) is the most common type of skull fracture. The result of compression of the skull during delivery, a linear skull fracture most often has no associated injuries and causes no symptoms. Bleeding may be seen extracranially (common) or intracranially (rare). Intracranial bleeding causes symptoms referable to the bleeding rather than to the fracture itself. 35,61
The typical depressed skull fracture is of the “ping-pong” type, an indentation without loss of bony continuity. When forceps are used during delivery, the direct cause of injury may result but is often without complications or sequelae. When neurologic signs are present, direct cerebral injury, intracranial bleeding, or free bone fragments should be suspected. 35,61
DATA COLLECTION
A linear skull fracture usually produces no signs or symptoms unless intracranial bleeding has occurred. Skull x-ray films most frequently demonstrate a parietal fracture. A depressed skull fracture may be noted by presence of a visible depression or a palpable “ping-pong” fracture in the parietal or temporal area. No other signs and symptoms are present unless intracranial bleeding or focal irritation of the cortex causes them. Evaluation with a skull x-ray examination or CT scan is necessary to delineate the fracture and to identify complications.
TREATMENT
No treatment is necessary for a linear skull fracture. Treatment of a depressed skull fracture varies and centers on the mode of treatment and the necessity of treatment for fractures that create no neurologic symptoms. If free bone fragments or clots are identified, neurosurgical intervention is necessary. More conservative approaches are indicated when no complications are present. Noninvasive treatments such as vacuum extractors and breast pumps have been used with success to raise the depressed bone segment. 61
COMPLICATIONS
With a linear skull fracture, the single complication to be aware of is a “growing” skull fracture. A dural tear may allow leptomeninges to extrude into the fracture site, setting up the possibility of a leptomeningeal cyst. As the cyst enlarges, the edges of the fracture may fail to fuse and even spread apart, giving the appearance of a “growing” fracture. Palpation and x-ray examination demonstrate the lesion. Surgical correction may be necessary to ensure healing and prevent further complications. With a depressed skull fracture, intracranial bleeding and direct cerebral injury with seizures or residual neurologic deficit are rare.
PARENT TEACHING
Parents should be instructed to have the fracture site monitored for several months to ensure that reunion of the bone has taken place. Patients will require no other aftercare unless neurosurgical intervention was necessary or complications developed.
Intracranial Birth Injuries
Three major forms of bleeding occur intracranially: epidural hematoma, subdural hemorrhage, and subarachnoid hemorrhage (see the Critical Findings box on p. 761). Added to these are cerebellar hemorrhages, cerebellar contusions, and cerebral contusions. Each has its own particular set of symptoms and signs and complications and sequelae. IVH usually is not related to trauma and is covered separately in this chapter.
PHYSIOLOGY AND ETIOLOGY
An epidural hematoma is pathophysiologically difficult to form in newborns because of a relatively thick dura. When present, it is almost always accompanied by a linear skull fracture across the middle meningeal artery.
Subdural hemorrhage is more common in term infants than in preterm infants and occurs from trauma tearing veins and venous sinuses. Although some assume its presence represents birth trauma, several authors indicate that this is not necessarily the case. 61,65 Subdural hemorrhage has been linked with maternal use of aspirin and also to maternal ingestion of phenobarbital. 61 Four major pathologic entities are defined: (1) laceration of the tentorium, (2) laceration of the falx, (3) laceration of the superficial cerebral vein, and (4) occipital osteodiastasis. Tentorial laceration causes a posterior fossa clot with compression of the brainstem. The straight sinus, Galen’s vein, lateral sinus, and infratentorial veins may be involved. Laceration of the falx is caused by rupture of the inferior sagittal sinus. The laceration usually occurs at the junction of the tentorium and the falx, and the clot appears in the longitudinal cerebral fissure over the corpus callosum. Laceration of superficial cerebral veins causes subdural bleeding over the convexity of the brain. Subarachnoid bleeding or contusion of the brain also may be present. 36,61
A subarachnoid hemorrhage is the most common type of neonatal intracranial hemorrhage. In term infants, trauma is the most common cause, whereas in preterm infants, hypoxia is more often the cause. Small hemorrhages are more common than massive ones and usually result from venous bleeding. Underlying contusion may be present. 3,36,61
Intracranial Birth Injuries
1. Epidural hematoma
a. Occurrence: Rare.
b. Location: Bleeding occurs into the epidural space. Blood is located between the inner area of skull bone and the periosteum.
c. Pathophysiology: Most (not all) with history of traumatic labor or delivery.
d. Clinical findings:
Increased intracranial pressure (swollen fontanel).
Seizures may occur.
e. Associated problems: Almost always accompanied by a linear skull fracture.
2. Subdural hemorrhage
a. Occurrence: More common in term infants than in preterm.
b. Location: Bleeding is produced from tear of cerebral vein or sinus, which is often accompanied by a tear in the dura. Exact location of the hematoma depends on the location of the bleeding source. 61
Laceration of the tentorium
Laceration of the falx
Laceration of the superficial cerebral vein
Occipital osteodiastasis
c. Pathophysiology:
Debate as to whether its presence indicates birth trauma. Volpe indicates that most cases result from trauma. 61
Linked to maternal use of aspirin and maternal ingestion of phenobarbital.
d. Clinical findings:
Neurologically abnormal at birth, if massive bleed:
Seizures
Stupor or coma
Skew deviation of eyes
Pupil changes: unequal pupils, poorly responsive pupils, fixed and dilated pupils
Nuchal rigidity
Apnea and bradycardia
Signs of increased intracranial pressure
e. Associated problems: Risk for herniation with lumbar puncture.
3. Subarachnoid hemorrhage
a. Occurrence: Most common type of neonatal intracranial hemorrhage.
b. Location: Blood is within the subarachnoid space but not because of extension from other areas. Small hemorrhages are more common than large ones. Source believed to be small vascular channels. 61
c. Pathophysiology:
Term: Usually caused by trauma
Preterm: Usually caused by hypoxia
d. Clinical findings:
Most common: Minimal or no symptoms
Buy Membership for Neonatal and Perinatal Medicine Category to continue reading. Learn more here




