Cervical Squamous Intraepithelial Lesions
Introduction
Human papillomavirus (HPV) infection is now understood to be the underlying cause of squamous carcinogenesis in the cervix.1–4 Older diagnostic classifications of preinvasive disease based purely on descriptive correlation of histology with clinical behavior included dysplasia/carcinoma in situ (CIS; a four-grade system) and cervical intraepithelial neoplasia (CIN; a three-grade system). Each provided a convenient diagnostic spectrum against which patient samples could be matched, and both are still in use to varying degrees.
The clinical goal of segregating individual lesions into dichotomous high- and low-risk categories was furthered by evidence showing that cancer outcomes correlated predominantly with one of two HPV subtype classes. Thus, the two-class Bethesda System of low-grade squamous intraepithelial lesion (LSIL) and high-grade squamous intraepithelial lesion (HSIL) was formally endorsed by the National Cancer Institute (USA) at a workshop held in December 1988.5 Implementation was recommended for lesions in the cervix and vagina. LSIL was generally equated with condylomata and CIN 1, and HSIL with CIN grades 2 and 3 (CIN 2, CIN 3, or CIN 2–3). This principle of a two-tier system was reaffirmed by consensus of the College of American Pathologists and American Society for Clinical Pathology (ASCP) in 2012, with the additional recommendation that it be extended to all anogenital HPV-related lesions, including those in vulvar and perianal sites.6
The initial expectation of the two-tier system was that viral type would be the primary determinant of outcome, and careful correlation of intraepithelial morphology with viral type would yield diagnostic criteria for the new entities of LSIL and HSIL. However, it is now clear that LSIL is the biologic manifestation of productive HPV infection with episomal viral DNA. Therefore, all HPVs can generate low-grade morphology as this type of cellular differentiation is required for viral replication to produce viral particles (virions). These infections and their cytohistologic manifestations are almost always transient, resolving on average in less than a year.7
HSIL results predominantly from genomic integration of high-risk types of HPV DNA into the host genome of replicating parabasal cells, with consequent deregulation of expression of E6 and E7 viral oncogenes. The parabasal cells become disorganized relative to the underlying basement membrane, with subsequent clonal expansion extending upward toward the epithelial surface (Figure 10.1). Cells containing only integrated viral DNA are virologically noninfectious as no viral particles are produced but the viral genes drive the human (host) cells to proliferate. HSILs may, however, contain both episomal and integrated HPV DNA,8 which is consistent with the presence of koilocytes in some HSILs.
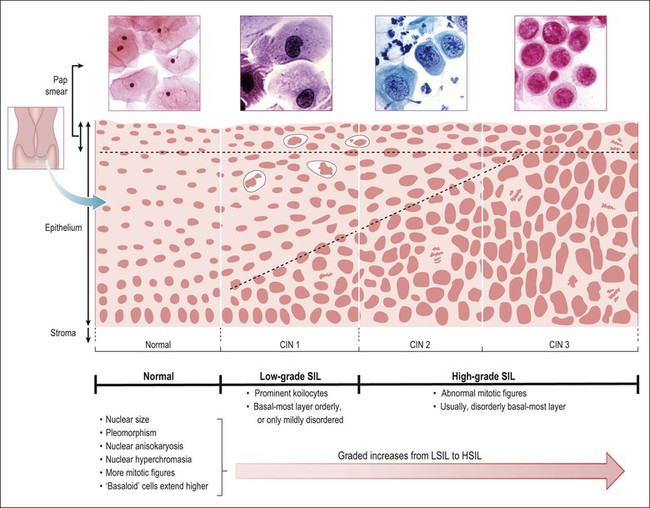
Figure 10.1 Morphologic features and nomenclature of preinvasive cervical disease. The morphologic changes that occur with increasing lesion grade and how the SIL (Bethesda) and CIN systems relate to one another are illustrated. Quantitative features that become increasingly more abnormal with increasing grade are listed, along with those qualitative features that differ across the LSIL–HSIL boundary. The corresponding cytologic smear appearances resulting from exfoliation of the most superficial cells are also illustrated. Note that some pathologists subdivide HSIL into HSIL (CIN 2) and HSIL (CIN 3), which are comparable to CIN 2 and CIN 3 respectively.
Of the more than 120 HPV types known to exist,9 only about 30–40 affect the genital tract. Probably less than 15 are oncogenic; the most common is HPV type 16 and its related viruses 31, 33, 35, and 56 from the α 9 clade (a taxonomic group derived from a common ancestor)9 and type 18 with its close relations such as type 45 (Table 10.1).10 They are termed high risk or oncogenic because they are the types found in invasive tumors. Progression of high-risk viral infection to HSIL is inefficient and, although high-risk types are the most common cervical HPV infections, most result in only low-grade lesions. The low-risk group constitutes only a minority of cervical infections. The low-risk HPV types are prototypically HPV types 6 and 11 whose biology is one of transient productive infection with only extremely rare examples of progression to carcinoma. The apparent prevalence of HPV infection in cervical lesions of different types and grades depends on the technique used for detection of the virus and the criteria applied for histologic annotation.
Table 10.1
Classification of HPV Types Associated with Genital Lesions10
| Most Common Types | |
| 6,11 | Condyloma acuminatum, LSIL (condyloma/CIN 1) |
| 16 | All grades of SIL, squamous cell carcinoma |
| 18 | All grades of SIL, adenocarcinoma, squamous cell carcinoma, small cell carcinoma |
| Less Common Types | |
| 31, 33, 35, 39, 45, 51, 52, 56 | All grades of SIL, squamous cell carcinoma |
| 30, 40, 58, 69 | All grades of SIL |
| 42, 43, 44 | Condyloma acuminatum, LSIL (condyloma/CIN 1) |
| 53 | Normal cervical epithelium, LSIL (condyloma/CIN 1) and sometimes HSIL (CIN 2) |
| 54 | Condyloma acuminatum |
| 55 | Bowenoid papulosis |
| 59 | Vulvar HSIL (usual type vulvar intraepithelial neoplasia) |
| 61, 62, 64, 67 | Vaginal HSIL (vaginal intraepithelial neoplasia) |
| 66 | Squamous cell carcinoma |
| 70 | Vulvar papilloma |
Irrespective of HPV type, the viral cytopathic effect (koilocytosis) and the production of viral capsid protein become progressively less frequent with increasing lesion grade (Table 10.2).11 Indeed, the inability of most high-grade lesions to support productive HPV infection can be viewed in a biologic context as viral failure. Local immune response within the cervical microenvironment is somewhat more common with high-risk HPV infections, and this can be associated with regression of HSILs.12,13 Conversely, low-grade lesions are, in a sense, ‘successful’ infections in that they represent productive infections with little or no propensity to kill the host.

Although SILs are capable of changing dynamically over time as a combined function of viral type(s), phase of viral life cycle (especially episomal vs integrated) and host factors, classification of SILs must be accomplished from the morphologic appearance of an individual HPV-infected squamous lesion. Further information about virologic and immunologic dynamics of HPV infection from individual and public health perspectives are available in Chapter 9. Cervical biopsy and cytologic smears each have their own sampling and interpretive errors, occasionally creating discordant results. Both are equally variable and may provide valuable information on disease presence or absence. Even visually directed colposcopic biopsy is imperfect in identifying the area of most severe pathology.14 Every attempt should be made to reconcile discordances by a combination of interpretive re-review, or further sampling, as clinically appropriate. Evidence-based criteria-driven approaches to diagnosis remain the best way to achieve clinical utility with a minimum of interpretive variation.15
Squamous Intraepithelial Lesions (SILs)
Nomenclature
The nomenclature used to describe the precursor conditions of invasive squamous cell carcinoma continues to be a subject of some debate. In the 1950s and into the 1960s, the term ‘dysplasia’ was equated to a graded lesion something less than CIS, which was diagnosed and managed separately. Both were composed of basal-type cells extending upward in the epithelium, to almost full thickness in the case of severe dysplasia. Flattening of the topmost surface cells, construed as a sign of differentiation, was said to occur in severe dysplasia, but not CIS. These diagnoses led to widely divergent interventions: the former passively followed, and the latter often to hysterectomy. Critical examination of the data subsequently showed that distinction between severe dysplasia and CIS was not only poorly reproducible by pathologists, but, when applied, failed to stratify patients into differing risk groups for invasive carcinoma.15,16 Lack of clinical significance of the dysplasia/CIS distinction led to the simplified classification of CIN in which three grades of precancerous lesions were acknowledged, but the term ‘carcinoma’ was reserved for invasive processes. New treatment options for intraepithelial precursor lesions, intended to ablate only the cervical lining, were introduced. These included topically applied liquid nitrogen (cryosurgery), laser ablation, and local excision by electrocautery loop.
Knowledge of the role of HPV infection (see Chapter 9)1,2,15 and more specifically the roles of individual HPV types, suggested division according to the presence of the low-risk HPV types such as HPV 6 and 11 and the high-risk HPV types, most commonly HPV 16 and 18. Since the late 1980s, the Bethesda classification scheme, introduced for use in reporting cervical cytology smears, has incorporated these concepts into a bimodal classification system of LSIL/HSIL, which differ in their risk for subsequent carcinoma. HPV lesions previously considered condylomata or CIN 1 (mild dysplasia) are grouped into the single category of LSIL. These low-grade lesions have a low growth fraction, koilocytotic atypia (also called ‘HPV cytopathic effect’), and are the morphologic manifestation of productive HPV infection. They might perhaps be better called ‘low risk for the development of high-grade intraepithelial neoplasia or invasive carcinoma.’ All HPV types functionally produce LSIL at some point in their life cycle (or they would not survive). In contrast, HSILs are the approximate equivalent of CIN 2 and CIN 3 (moderate dysplasia, severe dysplasia, and CIS). HSIL is sometimes subdivided into HSIL-2 and HSIL-3 to reflect this comparison with CIN 2 and CIN 3. The relationship between these various terms is shown in Figure 10.1. A strength of the Bethesda System is that it may be applied to both cytologic and histologic specimens. The cells from an HPV-associated lesion are all included under the umbrella of SIL, as there is no underlying biologic or diagnostic basis to maintain a separate category of non-SIL condyloma.15 As suggested earlier, the concept of progression is best considered probabilistically, incorporating independent assessment of the results of cytology and biopsy and, when appropriate, HPV testing.17,18
Features
The histopathologic assessment of a cervical biopsy must determine whether SIL is present in a sample of epithelium and, if so, the grade of SIL (Figure 10.2). Both of these decisions may be difficult to make: the former because benign and reactive changes may be mistaken for SIL; the latter because interpretation of features used for grading is complex (Table 10.3).
Table 10.3
Histopathologic Features of SIL/CIN
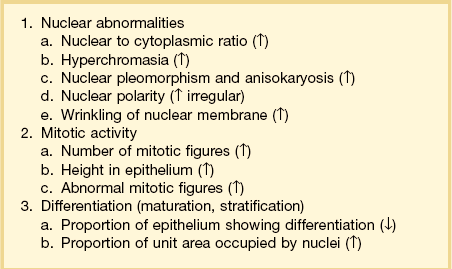
These features become progressively more prominent with increasing grade.
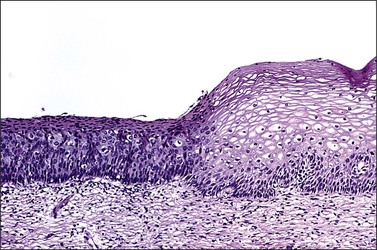
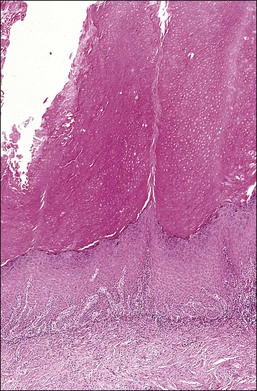
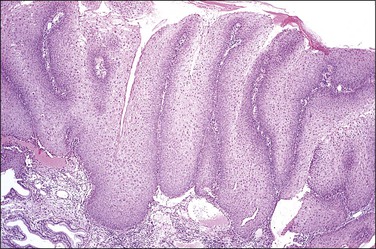
Figure 10.2 Abrupt transition between normal squamous epithelium (right) and an adjacent HSIL (left).
Changes of HPV Infection
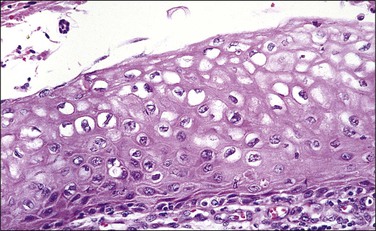
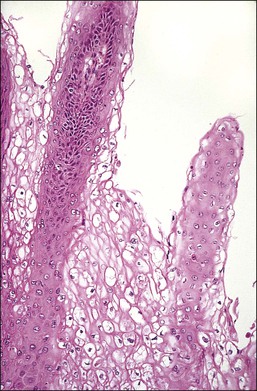
In cervical epithelia, all productive HPV infections commonly manifest themselves both cytologically and histologically through a distinctive cytopathic effect. The cell in which this is found has been termed the ‘koilocyte’ (Figure 10.3). This feature, first recognized more than 50 years ago, was given the term ‘koilocytotic atypia’ (some use koilocytic) as these cells histologically resembled those in skin warts. Some 20 years later it was recognized that this same cell type occurred in genital warts and was associated with both HPV infection and preinvasive squamous intraepithelial lesions.
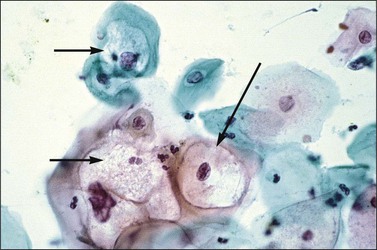
The koilocyte is an intermediate cell that has a prominent cytoplasmic space around an atypical nucleus (Table 10.4; Figures 10.3–10.8). Due to an extensively marginated cytoplasm, the halo has a sharp edge. The cytoplasmic change is thought to be due to abundant expression of the HPV E1∧E4 fusion protein, which binds with cytoplasmic keratin. Even in the state where the nuclei are not overtly dysplastic by size criteria, they are still, nonetheless, irregular and hyperchromatic and, if near the surface, may show a wrinkled nuclear membrane. The nuclei, which lack nucleoli, are usually two to four times larger in nuclear area than those of the adjacent, nonballooned cells. Koilocytotic atypia, which under the Bethesda classification is considered a low-grade SIL, is the most common definite abnormality in cytologically screened women and is found in up to 4% of all cervical smears.
Table 10.4
Koilocytotic Change: Diagnostic Criteria
Well-defined and exaggerated perinuclear halo
Cytoplasmic condensation around the halo
Nuclear area at least 2–3 times that of a normal intermediate cell nucleus
Increased nuclear to cytoplasmic ratio
Mild nuclear hyperchromasia (usually)
Wrinkled nuclear membrane
Nuclear membrane chromatin condensation
Degenerative nuclear changes (variable)
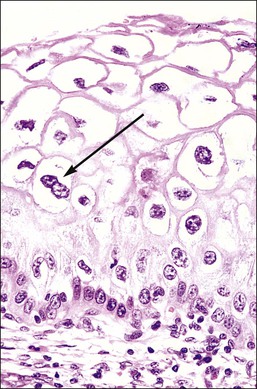
Figure 10.4 HPV-associated koilocytes in an LSIL. The cells in the intermediate layers are ballooned with copious clear cytoplasm. One cell is binucleate (arrow). The lowermost layer of cells against the basement membrane is orderly.
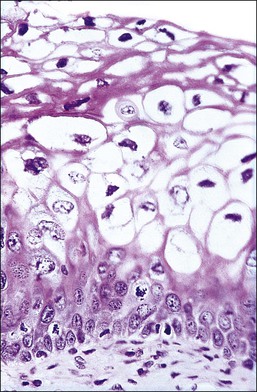
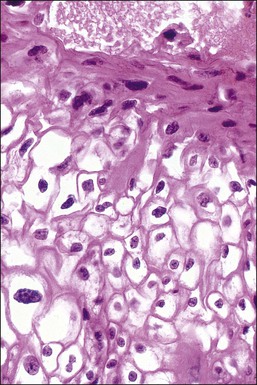
Figure 10.6 LSIL (CIN 1). Several of the koilocytes show nuclear atypia, which persists in the parakeratotic scale. Figures 10.4–10.6 are all low-risk viral lesions.
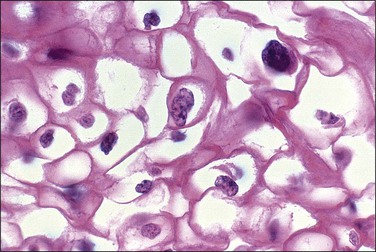
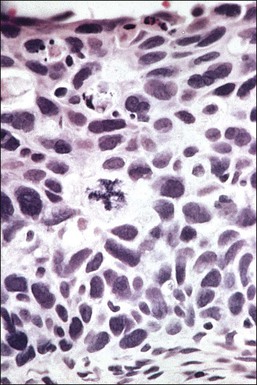
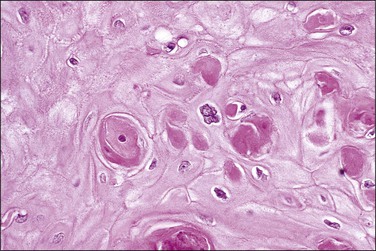
Figure 10.7 The nuclei of koilocytes are wrinkled and enlarged but show neither mitotic activity nor nucleoli.
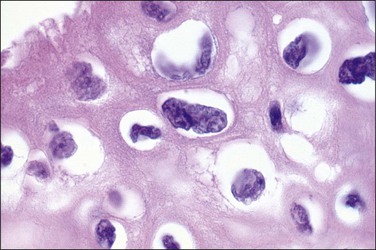
Figure 10.8 High-power magnification of koilocytes. The nuclei are wrinkled and enlarged with coarse chromatin.
While the koilocyte is often described to be pathognomonic for HPV infection, perinuclear halos that mimic koilocytotic atypia may be caused by other infectious diseases and at times may be due to artifact. Epstein–Barr virus, when present in the cervix, may be associated with koilocytic change19 (although this may also be due to coinfection with HPV). Likewise, when the cytoplasmic halo is less than morphologically perfect, i.e., when the borders are smooth or when the nuclei have smooth borders, trichomoniasis may be a consideration. It is therefore important that the presence of a cytoplasmic halo is not overinterpreted as due to HPV infection. Rather, it is the combination of a well-defined halo plus definite nuclear atypia as defined previously that confers specificity to the morphologic findings. Other features associated with HPV infection include binucleation (Figure 10.4) and meganuclei. Both are found in the mid to superficial levels. Some investigators have suggested that the latter feature, or more severely pleomorphic koilocytes, is more associated with high-risk HPV types. However, since over 85% of cervical HPV infections are due to viruses from the high-risk group, this is not a practically useful concept and LSILs of the cervix cannot be reliably genotyped by morphology.
Nuclear Abnormalities
The defining hallmarks of SIL are its nuclear abnormalities. These include nuclei that are enlarged, pleomorphic (irregular in size and shape), and often have a wrinkled nuclear membrane. The chromatin is increased in amount (hyperchromasia) and irregularly clumped, often condensing along the inside of the nuclear membrane. Collectively, this constellation of features is described as ‘nuclear atypia.’ These changes may reflect the polyploid and/or aneuploid DNA content of the cells induced by the action of HPV E6 and E7 on host DNA synthesis and cell cycle checkpoints (see Chapter 9) and are important for the diagnosis of SIL. Neoplastic atypia is distinguished from reactive changes by the heterogeneity of the nuclear changes in SIL, contrasting with the relatively homogeneous changes in reactive atypia. It is of note that nucleoli are rare in preinvasive lesions, especially in smears, but are commonly seen in reactive atypia.
Mitotic Activity
Mitotic activity above the basal layer, however, is not always by itself pathognomonic for SIL. A reactive or inflamed but otherwise normal differentiated epithelium may also have increased mitotic activity, but the mitotic figures are concentrated in the basal areas. More problematic are reactive changes in metaplastic squamous areas, such as an inflamed transformation zone, as these may have full thickness mitotic activity and fail to demonstrate the polarization of differentiation. The presence of reactive cytologic features lacking the particular chromatin condensation of SIL may assist in the distinction. Special stains for p16, which is positive in epithelia infected with high-risk HPV, may also be helpful in differentiating between reactive metaplasia and SIL.
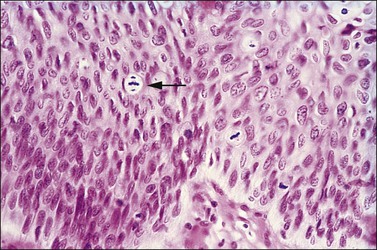
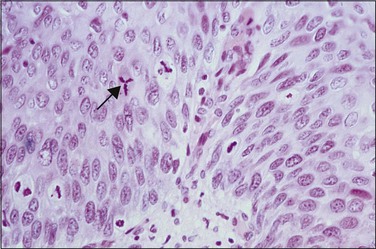
Abnormal mitotic configurations, which reflect aneuploidy, are common in HSIL, where they account for between 15% and 30% of total mitoses, but rare in LSIL. HSIL associated with HPV type 16 infection has the highest number of mitoses and the most abnormal forms.20,21 The most common of these abnormal configurations is the lag-type mitosis, which is defined as a metaphase with nonattached chromatin in the area of the mitotic figure. The ‘three-group metaphase’ (Figure 10.9), which is where the main mass of the chromatin aligns along the equatorial plate and the nonattached condensed chromatin remains laterally at the two polar sites, has been found in 6% of CIN 1–2, 56% of CIN 3, and 93% of high-grade CIN lesions just adjacent to microinvasive carcinoma.22,23 Two-group metaphases (displaced chromatin at only one polar site) may also be seen. Less common than either of these forms is the multipolar mitotic figure, either as a triaster (tripolar) (Figure 10.10) or as a more bizarre multipolar figure (Figure 10.11). Tripolar mitoses may reflect polyploidy, rather than aneuploidy, and thus may be seen in both HSIL and LSIL.
Differentiation, Maturation, and Stratification
The proportion of epithelial cells showing differentiation is a useful indicator of the grade of SIL, although it must not be taken as the only criterion. For example, while SIL develops by a dysplastic process and may show little if any differentiation, it may be difficult to distinguish from an immature, but nondysplastic metaplastic squamous epithelium that also lacks any substantial degree of cytoplasmic differentiation. In this case, the distinguishing feature is the lack of nuclear atypia in the metaplastic process as well as much less evidence of mitotic activity. Nonetheless, distinction between the two conditions can be difficult and the presence of atypical changes in immature metaplastic squamous epithelium may indicate SIL, as shown by the presence of high-risk HPV types, high Ki-67 proliferation indices, p16 expression, and follow-up studies.24,25
As normal cells differentiate and mature and migrate toward the surface, stratification is observed. One means of assessing maturation is to look for a decreasing percentage of nuclear area to overall epithelial area, reflecting a decreasing nuclear to cytoplasmic ratio at increasingly more superficial levels of the epithelium. In smears, which sample superficial cell layers preferentially, this change in ratio is quite dramatic. In normal smears, the nucleus has undergone pyknosis by the time the cell reaches the surface, so that in the smear the nuclear to cytoplasmic ratio is quite low. With increasing grade of SIL, the individual cells have matured progressively less so that the amount of cytoplasm present, as well as its differentiation, is less. Thus, mildly dyskaryotic (a synonym of dysplasia used in cytologic terminology)/LSIL cells present in cervical smears/scrapes have ample cytoplasm with a well-defined polygonal squamous shape, and moderately dyskaryotic/HSIL-2 cells possess less cytoplasm and a less well-defined oval or elliptical squamous shape, whereas in severely dyskaryotic/HSIL-3 cells the rim of cytoplasm that encircles the nucleus is small. These features also occur in histopathologically defined lesions and, in SIL, the proportionally decreasing quantity of cytoplasm contributes far more to the increase in the nuclear to cytoplasmic ratio with increasing lesion grade than does the change in nuclear size. This is consistent with the persistence of nuclear abnormality throughout the epithelial thickness in all grades of SIL.
Disease States: Types of SIL
Despite the earlier critical comments about reproducibility, application of discrete diagnostic criteria allows for distinction between benign cervix and SIL, and grading of SILs. SIL is primarily divided into two major classes of LSIL (condyloma/CIN 1) and HSIL (CIN 2–3), using similar terminologies across cytologic and histologic specimens.6
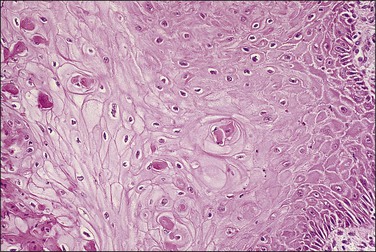
The following discussion should be used as a general guide to the central features of the distinct grades of SIL, since examples of the same SIL grade may have varying appearances. For example, one specimen may show a lack of differentiation and stratification throughout (Figure 10.12), whereas others may show more prominent mitoses, some being abnormal (Figure 10.13), or bizarre nuclei located at superficial levels (Figure 10.14). Many of the histologic features used in the grading of SIL may vary independently of each other, so the emphasis put on each of these criteria may vary from one specimen to another. All of this variation diminishes reproducibility of diagnosis.
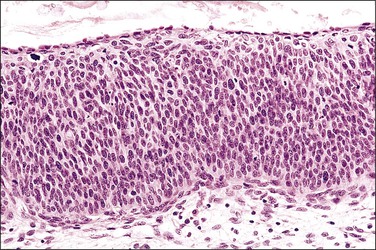
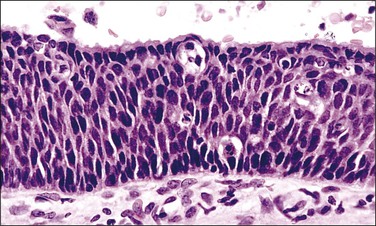
Figure 10.13 HSIL (CIN 3) in which a thin residual layer of mucinous columnar cells is present on the surface.
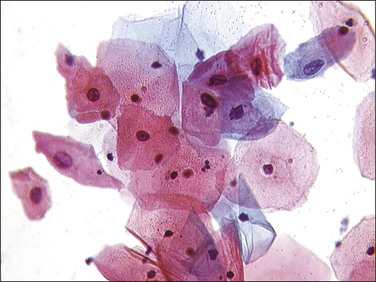
Like histology, assignment of an overall grade of SIL to a smear is as subjective as the assessment-based examination of the individual cells. The cervical smear will frequently contain cells showing both grades of SIL, and it is the most severe cell type that determines the grade (Figure 10.15). A smear containing only a few dyskaryotic (dysplastic) cells, all of which show a marked degree of abnormality, almost certainly reflects HSIL. Likewise, a smear containing a majority of dyskaryotic (dysplastic) cells of moderate degree with only occasional severely dyskaryotic (dysplastic) cells, while seemingly suggestive of HSIL (CIN 2), will often disclose HSIL (CIN 3) on biopsy or conization.
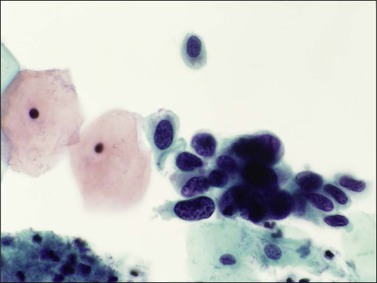
Figure 10.15 HSIL, severe dyskaryosis, on a cervical smear. The atypical cells have a high nuclear to cytoplasmic ratio.
LSIL (Condyloma/CIN 1)
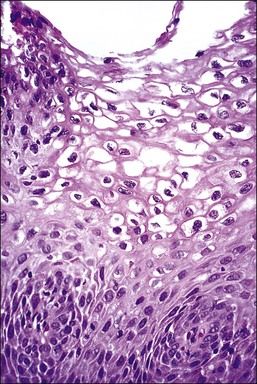
LSIL is a term that unifies entities previously referred to as condyloma acuminatum, ‘flat condyloma,’ and CIN 1. LSIL is the histopathologic presentation of productive episomal HPV propagation, essentially a field effect caused by viral activation in maturing squamous cells. Although a degree of nuclear maturation occurs, abnormal nuclei persist throughout the full thickness of the epithelium (if this were not so, a diagnosis by cytologic smear would not be possible; see earlier sections) (Figures 10.16–10.18). Mitotic figures, if present, are few in number and generally confined to the basal third of the epithelium. Abnormal mitosis forms are uncommon: these usually indicate aneuploidy and thus are more specific for the diagnosis of HSIL. Characteristic LSIL changes are concentrated in the upper part of the epithelium where productive episomal virus propagation in maturing squamous cells forms characteristic koilocytes. These koilocytotic nuclei can be wildly pleomorphic, and are among the largest nuclei seen in any kind of SIL. Upon integration of viral DNA into the genome of host cells, episomal propagation, and their koilocytotic phenotype, are diminished. Thus koilocytes are less common in HSIL (CIN 2 and 3), although they do still occur in these lesions, particularly where surface epithelial maturation is retained. LSILs, on occasion, may lie adjacent to high-grade lesions, or occasionally even adjacent to carcinomas. Sometimes this reflects progression of a single viral infection from an episomal to integrated phase across one epithelium, whereas in others it may be due to infection by multiple viral types.
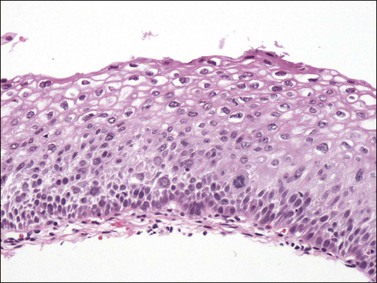
Figure 10.16 LSIL (CIN 1). Cytologic atypia extends throughout the epithelium but there is cytoplasmic maturation and the superficial-most epithelial cells display marked koilocytosis.
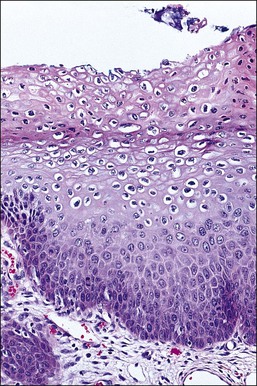
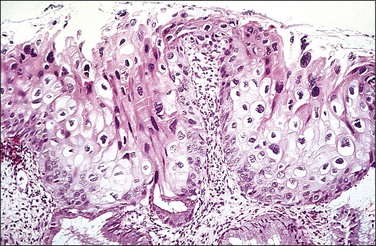
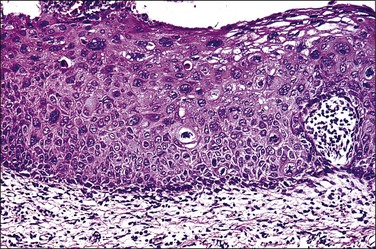
Figure 10.18 LSIL (CIN 1). There is prominent nuclear pleomorphism in koilocytes with extensive cytoplasmic maturation.
Several other features are found with low-grade lesions. Nuclei that are binucleate (Figure 10.4), or even sometimes multinucleate, are found in 95% of HPV infections.26 Occasional cells may show individual cell keratinization (dyskeratosis) (Figures 10.19 and 10.20). In smears, LSIL (mildly dyskaryotic) cells have ample cytoplasm with a well-defined squamous shape (Figure 10.21). Anucleate and nucleate keratinized cells are commonly present in sheets or plaques with poorly defined cell borders.
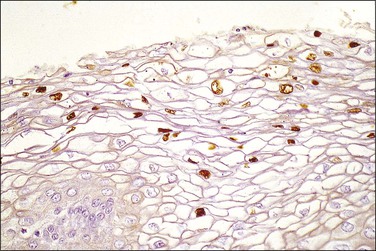
On a cellular basis, the koilocyte in histologic specimens is usually distinctive although the number of cells with koilocytotic change ranges from few to many (Figure 10.22). Typically, the nucleus is 3–4 times enlarged in area compared to a normal intermediate cell, uniform in size and shape, and has a halo with smooth outer borders. HPV immunostains have shown that typical koilocytes usually react with antibodies to the HPV L1 group-specific capsid protein (Figures 10.23 and 10.24). Since capsid/virion production is a temporally controlled phenomenon linked to both differentiation and lesional age, which likely explains the variability in koilocyte number between lesions, not all cells containing HPV will necessarily stain. Cells less typical for koilocytes are less likely to stain. Because of the potential social stigma often attached to a smear or biopsy specimen that is diagnosed as harboring HPV, prudence dictates that no specimen should be diagnosed as LSIL unless the overall microscopic picture is distinctive.
LSIL (Condyloma Acuminatum)
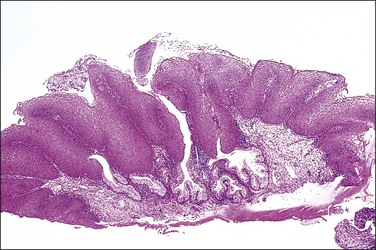
Condylomata acuminata of the cervix, exophytic papillary lesions caused by HPV (Figure 10.25), are much less common than those with flat architecture. This fact is consistent with the knowledge that the acuminate architecture is somewhat more frequently associated with HPV types 6 and 11 and some other low-risk types, and that these make up only 10–15% of cervical infections. Yet HPV 6/11 account for around 95% of cutaneous genital condylomata. Larger condylomata can be seen with the naked eye, and they may initially be mistaken for carcinoma (Figure 10.26).
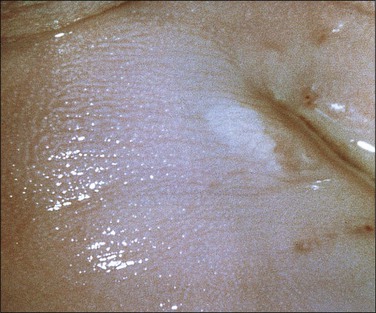
Figure 10.25 LSIL (condyloma acuminatum). The condyloma is exophytic but very small in size. It turned white when 3% acetic acid was applied.
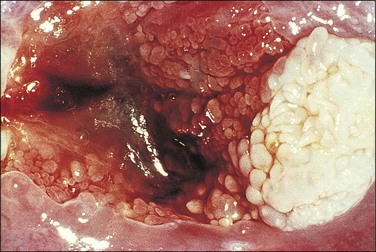
Figure 10.26 LSIL (condyloma acuminatum). This exophytic condyloma acuminatum is large and cauliflower-like.
The histology of exophytic, or acuminate, LSIL (condyloma) shows papillomatosis, acanthosis, parakeratosis, and hyperkeratosis. At higher magnification, each asperity, i.e., each papillary frond, has a tiny blood vessel at its core. Koilocytotic atypia is usually a prominent feature, with individual cell keratinization (dyskeratosis) and multinucleation. There is often a chronic inflammatory infiltrate in the underlying cervical stroma (Figures 10.27–10.30).

LSIL (‘Flat Condyloma’/CIN 1)
Flat LSILs that lack the architecture of condyloma acuminatum are recognizable colposcopically, cytologically, and histologically but cannot usually be seen with the naked eye (not to be confused with condylomata lata or flat warts of secondary syphilis, which are external genital lesions) (Figures 10.4–10.6, 10.16–10.18, 10.22–10.24). The colposcopic features are fully described later, but they are not altogether diagnostic. Based on histology, several features in addition to the presence of koilocytes are useful in the detection of HPV infection. On low-power magnification, large areas may be composed of squamous epithelial cells lacking glycogen. While suggestive, this feature is nonspecific. The cytoplasm from the basal-most cells to the surface is eosinophilic. Commonly a sharp boundary demarcates the epithelium that is glycogen rich (normal) and glycogen poor (HPV). In addition, the superficial cells in the glycogen-poor zones commonly show acanthosis, parakeratosis, and sometimes even hyperkeratosis. The last, rarely, may be quite striking (Figure 10.31). The term flat condyloma, originally used to describe lesions containing koilocytes but without a condylomatous architecture or CIN 1, is a contradiction and is no longer used, and is now replaced by LSIL. Whether flat lesions with and without CIN 1 can be separated reproducibly, and whether their separation has any clinical meaning, is debatable but some, particularly those using the CIN system, attempt to make this distinction.