Chapter 26 Achieving Functional Independence
Functional independence is the ability to perform daily living tasks without help. The achievement of functional independence ensures that individuals can participate fully in life situations that are meaningful and purposeful. Whether experiencing a physical disability or not, participation in activities of daily living or life occupations is essential to health and well-being.3 Anthropologists have noted that involvement in the daily routines of self-maintenance, production, and leisure enables humans to express themselves, establish relationships, and build self-identity.5 The World Health Organization has recognized the importance of participation in life situations to health by reframing the International Classification of Impairments, Disabilities, and Handicaps31 as the International Classification of Functioning, Disability and Health.30 In doing this, understandings of health have shifted significantly from definitions relating to the absence of disease or impairment. This embraces the notion of an individual engaging with and functioning in her or his world even with the presence of a disability and physical challenges. Supporting this shift is emerging evidence of the powerful therapeutic benefit of participation in meaningful daily occupations.5 Individuals who are able to achieve meaningful participation in life situations are more likely to experience and report increased personal satisfaction and quality of life, increased levels of energy, fewer physical ailments, reduced pain, and improved physical functioning.17 Ultimately, this impact can decrease the costs of health associated with burden of care, the treatment of physical symptomatology, and poor emotional health.
The goal of medical rehabilitation programs for persons experiencing physical disability as a result of injury, illness, or a developmental condition is to maximize functional independence over time.7 All members of the rehabilitation team are focused on restoring or enhancing functional capacity such that individuals can engage optimally in daily life tasks that are meaningful and purposeful. Because of the subjective nature of what constitutes “meaningful” and “purposeful,” it is important to adopt a family- or client-centered frame of reference for care. This frame of reference defines a set of philosophies, attitudes, and approaches to care for persons with special needs and their families.8 It refers to a relationship between the person, family, and health care professional that builds on the person’s and family’s priorities and that responds to their mutual goals.4 Some key elements in family- or client-centered care include recognizing family strengths, respecting different methods of coping, facilitating family and professional collaboration at all levels of health care, and sharing complete and unbiased information with families on a continuing basis and in a supportive manner. By adopting this frame of reference in practice, the rehabilitation team will be able to plan an evaluation and treatment process that matches the individual’s life goals and priorities. Rehabilitation programs that focus their interventions in this way are more likely to achieve the desired outcomes of enhancing productive living, promoting efficient recovery, and reducing the burden of care for individuals with physical disabilities over the long term.10,16,26
Evaluation
Using a family- or client-centered approach, evaluation of an individual’s functional independence necessarily begins with the determination of that person’s life goals, premorbid roles and activities, priorities for recovery, and contextual or cultural influences. From here, a more specific assessment can be conducted that evaluates the individual’s actual performance abilities and limitations in key areas of function. It also measures components of functional skill, including strength, range of motion, tone, sensation, balance, coordination, visual perception, and cognition. This type of evaluation process is referred to as the top-down approach and is considered “the best fit for the emerging system of health-care delivery.”14 The top-down approach has the advantage of focusing clearly on the roles and activities that are meaningful for patients, which increases motivation for participation in the rehabilitation process and increases the understanding of the relevance of rehabilitation to daily life. The top-down evaluation approach also allows for documentation of outcomes of rehabilitation in terms that are most likely to receive maximum reimbursement. Payers specifically seek outcomes of therapy that allow the patient to function most efficiently and effectively in daily contexts.14 Top-down evaluation results in the medical team addressing rehabilitation goals that are directly related to the individual’s performance in life roles.
Evaluating Meaningful Life Roles and Activities
Assessment of a person’s life goals, valued functional roles and activities, and priorities for recovery is a complex one. Because of the subjective nature of the content, there are few evaluation tools that provide the rehabilitation team with succinct, quantifiable data relating to this issue. Information about the person’s priorities and premorbid activity is usually gained through discussion and interview with the person and/or caregivers. It is important that those team members charged with the responsibility of gathering this information are skilled in techniques of interviewing and counseling to ensure that the individual is able to clearly communicate personal needs and wants.
Within the field of occupational therapy, an evaluation tool has been developed specifically for the purpose of assisting occupational therapists to establish occupational performance (functional performance) goals and priorities with their clients. The Canadian Occupational Performance Measure (COPM)18 was developed using a client-centered frame of reference and consists of a semistructured interview approach for gathering patients’ perspectives on their needs and wants in areas of self-care, productive living, and leisure. The evaluation process encourages patients to rate their perceptions of their current levels of performance and satisfaction with participation in key functional tasks. These are then reevaluated and rerated at the end of the rehabilitative process to provide outcome data relating to the patient’s perspective on recovery. Evaluation tools such as the COPM provide broad, descriptive information about the person’s functional independence needs, which allows the rehabilitation team to target specific areas requiring further evaluation and focus in treatment.
Evaluating Specific Performance Abilities
Once the patient’s valued life roles and activities have been identified and goals for rehabilitation determined, more specific evaluations are then completed to establish what performance limitations and abilities exist. A variety of methods can be used to assess functional skills. In many cases, therapists use guided observation and task analysis to determine the level of functional independence demonstrated by the patient. A number of formal measures have been developed for the purpose of measuring functional capacity. The most commonly used tool in this area is the functional independence measure (FIM).2 The FIM consists of 18 items examining the functional areas of self-care, sphincter control, transfers, locomotion, communication, and social cognition. Scores on the FIM provide an indicator of level of disability within motor and cognitive domains based on the level of assistance a patient requires to perform key functional tasks.21 A pediatric version of the FIM, the WeeFIM,1 has been developed for children aged 6 months to 7 years. It uses a similar structure to the FIM but modifies the items to account for developmental differences in social cognition and communication domains. Data from the FIM and the WeeFIM are being compiled in the Uniform Data System for Medical Rehabilitation to provide a repository of information regarding the functional independence of adults and children experiencing physical disability. Other tools used in rehabilitation settings to measure the functional abilities of patients include the following:
Evaluation of Components of Performance
Treatment
A number of treatment approaches can be used to assist an individual experiencing physical disability to achieve functional independence. The treatment approach chosen by the therapist and team depends on the specific goals set by the individual, the degree of functional limitation experienced, and the type and severity of the component skill impairments noted. Multiple treatment approaches can be used simultaneously with an individual to address different goals. Treatment approaches can generally be understood to fall into two main categories: restorative or compensatory.14 The goal of a restorative or facilitatory treatment approach is to restore the person’s capacity to perform functional skills by restoring the impaired component skills. The aim of this approach is to retrain the individual to perform functional tasks in the same way as was done premorbidly. It is an appropriate treatment strategy when complete or close to complete recovery is expected and few environmental or contextual barriers to functional independence exist. A number of frames of reference for intervention can be adopted depending on the impairments experienced by the individual. The most common frames of reference used in physical rehabilitation are as follows:
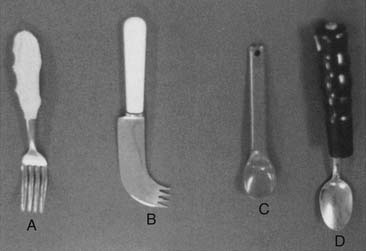
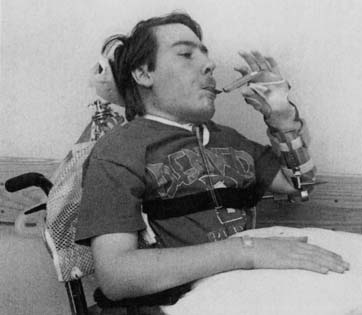
With the enormous progress made in recent years in technology, individuals with physical disabilities are now able to achieve much higher levels of functional independence than was previously possible through the use of technologic aids. The area of assistive technology is a dedicated field within rehabilitation that specializes in fitting individuals with physical and cognitive disabilities with both low- and high-tech solutions to enhance mobility, communication, community access, and learning. The application of assistive technology in physical disability is discussed in Chapters 17 and 23 of this text.